

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Fine-needle aspiration (FNA) cytology is the gold-standard diagnostic method for the preoperative diagnosis of thyroid nodules [12]. Although thyroid aspiration cytology using a large needle was initially introduced in the 1920s, FNA using a 23- to 27-gauge needle has been a mainstream diagnostic modality in the triage of thyroid nodules since the 1980s in most countries because of its diagnostic accuracy and safety [34567]. Core needle biopsy (CNB) of the thyroid was first introduced as an alternative to FNA in the 1990s [4] and is now widely used for the preoperative examination of thyroid nodules in Korea, with excellent results, because of advances in core needle devices (thinner needles and automatic devices), biopsy technology (new sampling technique) and ultrasound machine (high resolution) [8]. In this review, we present an overview of the indications, complications, and pathologic classification of thyroid CNB.
Go to : 
CURRENT GUIDELINES AND RECOMMENDATIONS
As evidence has accumulated regarding thyroid CNB, the Korean Society of Thyroid Radiology (KSThR) released its 2016 thyroid CNB guidelines [9]. These guidelines include recommendations regarding indications and complications, and are summarized in Table 1. A consensus statement on the pathology reporting system for thyroid CNB was published by the Korean Endocrine Pathology Thyroid Core Needle Biopsy Study Group in 2015 [10]. The six categorical diagnoses used in the Bethesda System for Reporting Thyroid Cytopathology (TBSRTC) were retained in the reporting system for thyroid CNB in order to ensure effective communication between pathologists and clinicians, with less likelihood of misinterpreting the pathologic results [110].
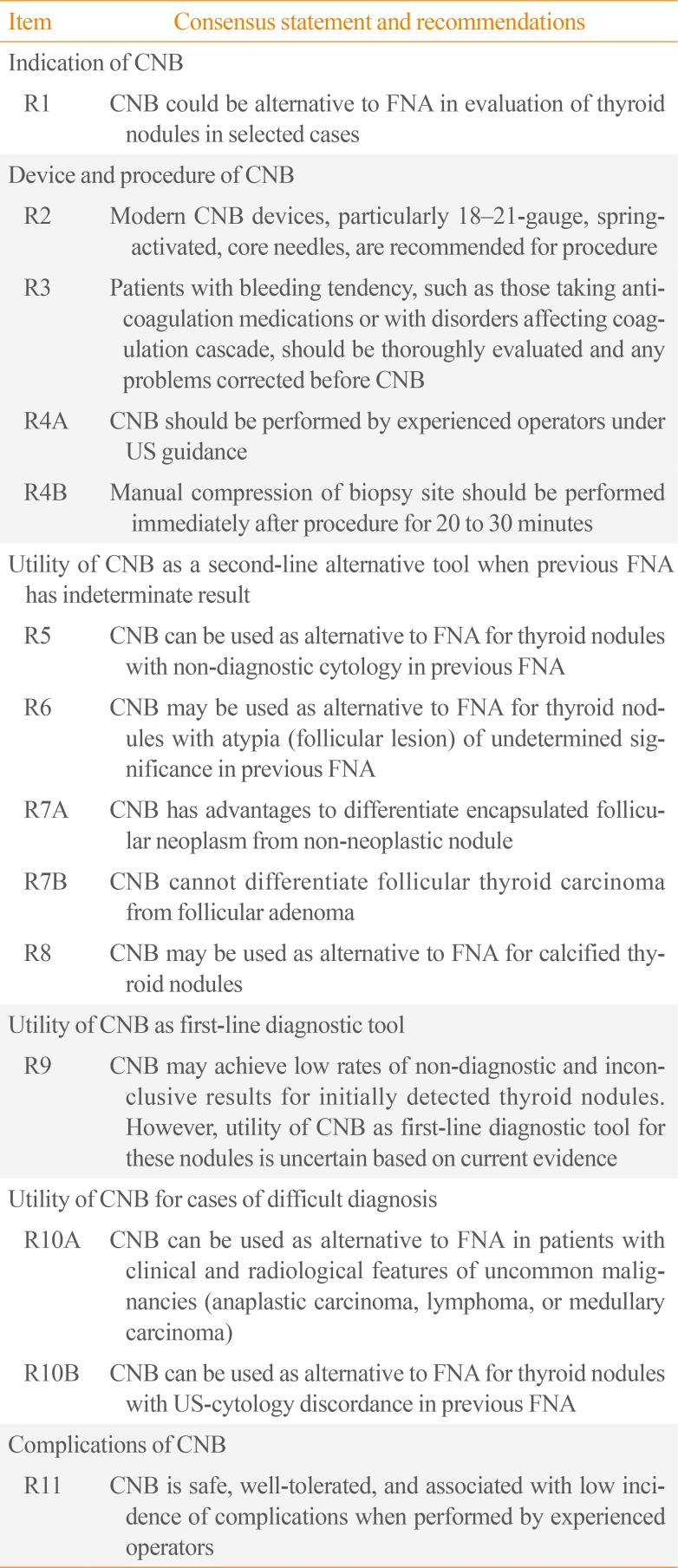
Table 1
Consensus Statement and Recommendations on Thyroid CNB from the Korean Society of Thyroid Radiology [9]
![]()
The current thyroid guidelines of the American Association of Clinical Endocrinologists/American College of Endocrinology/Associazione Medici Endocrinologi, British Thyroid Association, and KSThR permit the limited use of CNB for thyroid nodules, whereas the American Thyroid Association does not recommend CNB [2911].
Go to :
INDICATIONS
The most widely accepted indications for CNB in the literature include previous FNA results of non-diagnostic [12131415] and atypia of undetermined significance [151617]. The tissue obtained by CNB provides more abundant material than FNA cytology, especially in cases with marked sclerosis and calcification. A recent meta-analysis of published data showed that the non-diagnostic and inconclusive rates of CNB were 5.5% (95% confidence interval [CI], 2.2% to 8.7%) and 8.0% (95% CI, 4.4% to 11.5%), respectively, whereas the non-diagnostic and inconclusive rates of FNA were 22.6% (95% CI, 12.2% to 33.0%) and 40.2% (95% CI, 25.1% to 55.3%), respectively [18]. In another meta-analysis of thyroid nodules with initially non-diagnostic FNA results, the non-diagnostic rate (6.4%; 95% CI, 3.3% to 16.1%) of follow-up CNB was significantly lower than that of repeated FNA (36.5%; 95% CI, 29.9% to 43.1%) [13]. In large cohort CNB studies, the false-negative rates of CNB ranged from 1% to 3% [192021].
Although CNB may not be the method of choice for all thyroid nodules, previous studies have demonstrated the advantages of histologic diagnoses made using CNB specimens over the cytological diagnosis using FNA for several specific diseases. Malignant lymphoma, medullary thyroid carcinoma, anaplastic thyroid carcinoma, and parathyroid lesions can be confirmatively diagnosed with CNB based on the histologic morphology in conjunction with immunohistochemistry [222324]. While calcified nodules and degenerating nodules are often diagnosed as unsatisfactory with FNA because of the aspiration of acellular or paucicellular material, scant cellular nodules can be diagnosed as specific disease entities with CNB (Fig. 1) [252627].
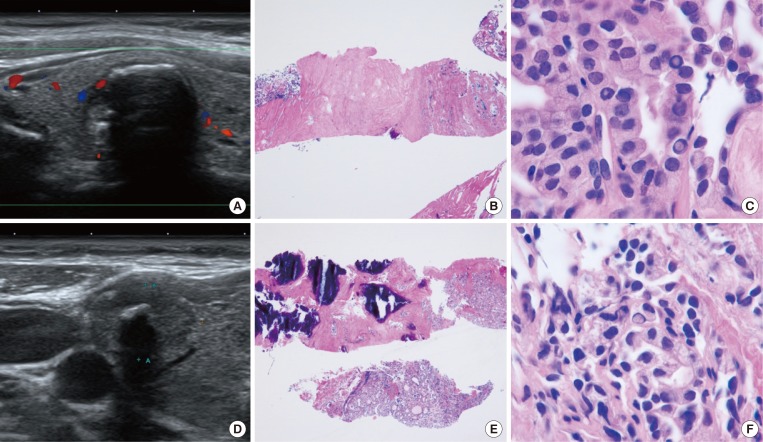 | Fig. 1Examples of core needle biopsy (CNB) in thyroid nodules with initial non-diagnostic fine-needle aspiration cytology. (A) On the ultrasound findings of case 1, there is a well-defined hypoechoic solid nodule with rim calcification. (B) CNB of the nodule shows scanty cellular and sclerotic nodules (H&E stain, ×40). (C) A high-power view shows the typical histologic features of papillary carcinoma (H&E stain, ×1,000). (D) An ultrasound image from case 2 shows a 1.5-cm, ill-defined hypoechoic solid nodule with macrocalcifications. (E) CNB shows marked calcification sclerosis, and focally follicular proliferative lesions (H&E stain, ×40). (F) A high-power view of the follicular lesion shows the histologic findings of papillary carcinoma (H&E stain, ×1,000).
|
Follicular-patterned lesions include nodular hyperplasia, follicular adenoma, noninvasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP), the follicular variant of papillary thyroid carcinoma (PTC), and follicular thyroid carcinoma. While FNA and CNB cannot differentiate follicular adenoma from follicular carcinoma and NIFTP from the invasive encapsulated follicular variant of PTC because vascular or capsular invasion cannot be assessed without surgery, it is possible to divide these follicular-patterned lesions into almost certainly benign non-neoplastic lesions and follicular newoplasms with a risk of malignancy. NIFTP and the follicular variant of PTC are diagnosed based on nuclear features in conjunction with architectural atypia showing a follicular growth pattern. For the diagnosis of follicular neoplasm with CNB, it is recommended that the tissue sampling of CNB should include tumor tissue, the tumor capsule, and adjacent normal parenchyma (Fig. 2).
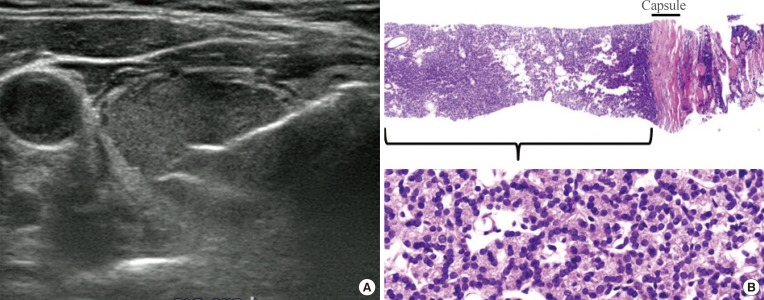 | Fig. 2Current core needle biopsy technique. (A) The specimen notch shown in ultrasound should include the tumor tissue, tumor capsule, and adjacent normal parenchyma. (B) Histologic examination of the specimen shows the tumor tissue with a microfollicular growth pattern, tumor capsule, and surrounding thyroid tissue (H&E stain, ×40, upper; ×400, lower). This case should be diagnosed as a follicular neoplasm.
|
A few studies have suggested that CNB is valuable as a first-line tool for diagnosing initially detected thyroid nodules [2128]. Suh et al. [21] reported that CNB had a non-diagnostic rate of 1.3% and an inconclusive result rate of 5.9%, a high diagnostic accuracy of 97.6%, and a complication rate of 0.2%.
Go to :
SAFETY AND COMPLICATIONS
The current thyroid guidelines suggest that CNB is a safe, tolerable procedure [1529]. The complication rate is also acceptable (0% to 4.1%), with a low rate of major complications (0% to 1.9%). Recently a large-population single-center study showed no procedure-related deaths, and low rates of major (0.06%) and minor (0.79%) complications [30]. To minimize complications, CNB should be performed by well-trained doctors under real-time ultrasound monitoring. Moreover, knowledge of the neck anatomy, anatomical variations, and potential complications is also required for the safe performance of CNB [31].
Go to :
PATHOLOGY REPORTING SYSTEM
The pathology reporting system of CNB is based on the six TBSRTC categories [10] and is summarized in Table 2. There is only one difference in terminology between the CNB reporting system and TBSRTC. The diagnostic category III for CNB is referred to as an “indeterminate lesion,” which corresponds to “atypia of undetermined significance” or “follicular lesion of undetermined significance” in TBSRTC. Subclassification based on the cytologic and/or architectural atypia in category III and IV was encouraged to enhance communication with clinicians and pathologists. Each diagnostic category in the TBSRTC has an implied risk of malignancy and clearly recommended clinical management steps regarding the triage of the patient for clinical follow-up, repeated FNA, or surgery. However, only limited data have been reported regarding the risk of malignancy in each diagnostic category of CNB.
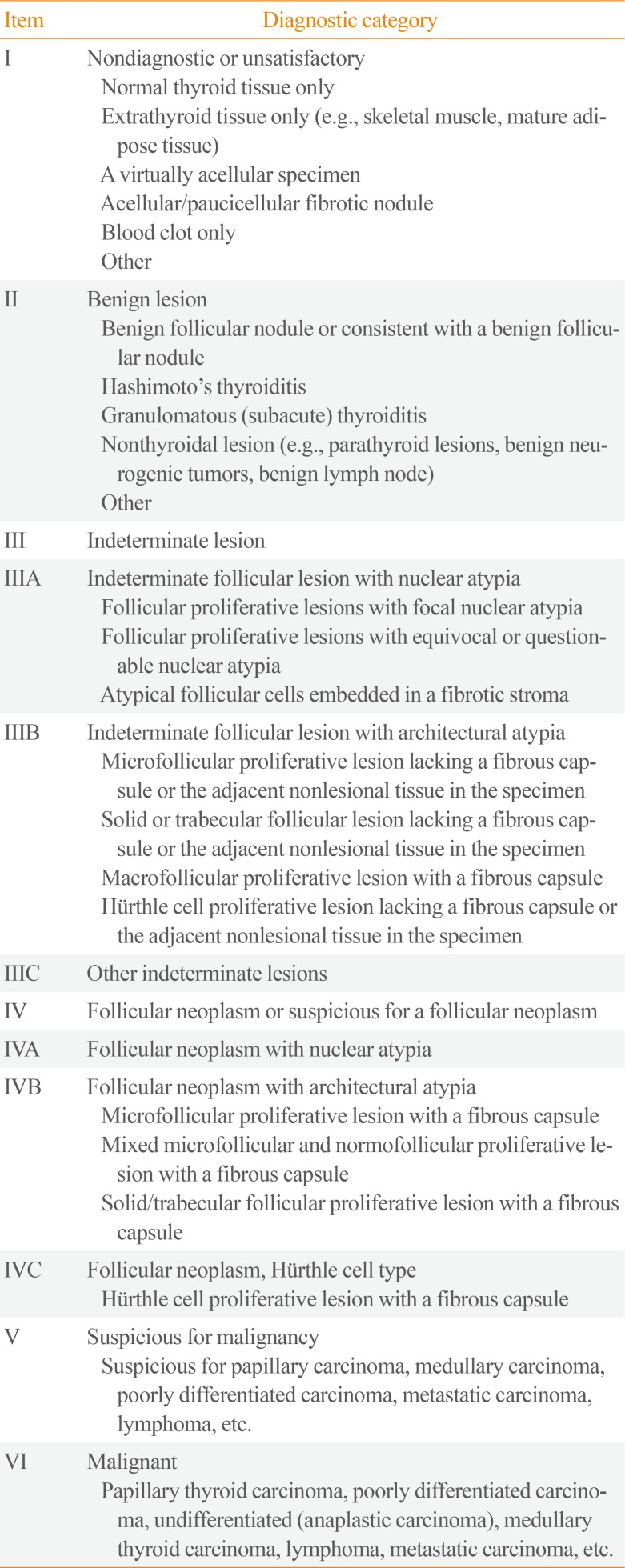
Table 2
Diagnostic Categories of Thyroid Core Needle Biopsy from the Korean Endocrine Pathology Thyroid Core Needle Biopsy Study Group [10]
![]()
Go to :
CONCLUSIONS
Thyroid CNB has been used as an alternative second option to FNA in patients with a previous non-diagnostic or indeterminate diagnosis, and is now suggested as a first-line tool for the diagnosis of thyroid nodule in selected cases. Recent studies have provided evidence for the efficacy and safety of thyroid CNB. Although the current thyroid CNB guidelines and pathologic reporting system are now widely available and affordable, further validation studies should be continued.
Go to :
 XML Download
XML Download