

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Calcium plays a number of critically important roles in physiology and pathology, in addition to its most widely recognised function as a critical structural component of bone. Many cells have calcium-sensing receptors, with evidence that the concentrations of calcium ions in the extracellular fluid directly regulate cell function (e.g., parathyroid, renal tubule, and many more). Extracellular calcium concentration directly impacts on cell membrane potentials, and so impacts on function of all excitable tissues, particularly the nervous system and the heart. Calcium is a key messenger in the contraction of muscle, including the myocardium. It is a co-factor for many enzymes and intimately involved in blood coagulation—indeed, calcium chelators (citrate, ethylenediaminetetraacetic acid [EDTA]) are the most commonly used anticoagulants in blood collection.
Bone is a connective tissue comprised primarily of type I collagen. Following the laying down of the collagen matrix by osteoblasts, deposition of calcium and phosphate ions to form hydroxyapatite crystals occurs between the collagen fibres. Bone is, thus, a composite material with tensile strength provided by collagen and compressive strength provided by hydroxyapatite. Bone mass is determined by the balance of bone-forming activity by osteoblasts and bone resorbing activity undertaken by osteoclasts. Bone formation is not directly influenced by calcium supply but in severe calcium deficiency that results in hypocalcaemia, mineralisation of osteoid can be impaired.
The role of calcium in vascular health is less clear-cut. There are calcium-sensing receptors on vascular smooth muscle cells and on platelets, calcium plays a role in smooth muscle contraction and its role in the electrophysiology of the heart and myocardial function have already been alluded to. Calcium deposition in the vasculature is a consistent feature of vascular disease and is predictive of adverse cardiovascular events. Indeed, calcium deposition in other soft tissues (such as the kidneys or muscles) has adverse effects on tissue function, and to prevent this there is a complex system of mineralisation inhibitors (such as pyrophosphate, fetuin-A, matrix GLA protein etc.). Obviously, tissue-specific targeting of mineralisation regulation is critically important so that mineralisation of bone is promoted but that of all other tissues is prevented. With ageing, the effectiveness of these mechanisms appears to decline, particularly in the vascular system. In addition, blood calcium levels appear to influence the development of vascular disease.
Go to : 
CIRCULATING CALCIUM IS A RISK FACTOR FOR VASCULAR DISEASE
There is a substantial literature which prospectively studies the association of circulating calcium levels with vascular disease and mortality. A recent meta-analysis found 11 prospective studies assessing the association between serum calcium and mortality [1]. Nine of these provided continuous risk estimates suitable for meta-analysis, which demonstrated a hazard ratio (HR) of death of 1.13 (95% confidence interval [CI], 1.09 to 1.18) for each standard deviation increase in serum calcium (approximately 0.1 mmol/L). These associations were attenuated in some studies after adjustment for cardiovascular risk factors such as circulating lipid levels, blood pressure, body mass index (BMI), etc. Some studies show serum calcium to be correlated with blood pressure and lipids but calcium remains an independent predictor of myocardial infarction after adjustment for these factors [2].
Many of these studies also prospectively assessed the association between serum calcium and myocardial infarction or cardiovascular disease, and meta-analyses of these findings are shown in Fig. 1 [1]. Again, risk is consistently increased across a range of geographies (Europe, North America, and Australasia) by about 10% per 0.1 mmol/L increment in baseline serum calcium. As for mortality, adjustment for cardiovascular risk factors attenuated but did not eliminate the associations, suggesting that these risk factors might mediate some of the relationship found. Circulating calcium as a predictor of stroke has been less extensively studied but Foley et al. [3], in a prospective study of almost 16,000 people over 12.6 years, found the HR of stroke increased 1.37 (95% CI, 1.28 to 1.46) per standard deviation of corrected calcium. These findings in normocalcaemic populations complement the body of evidence suggesting that hypercalcaemia is associated with increased mortality and cardiovascular disease [45].
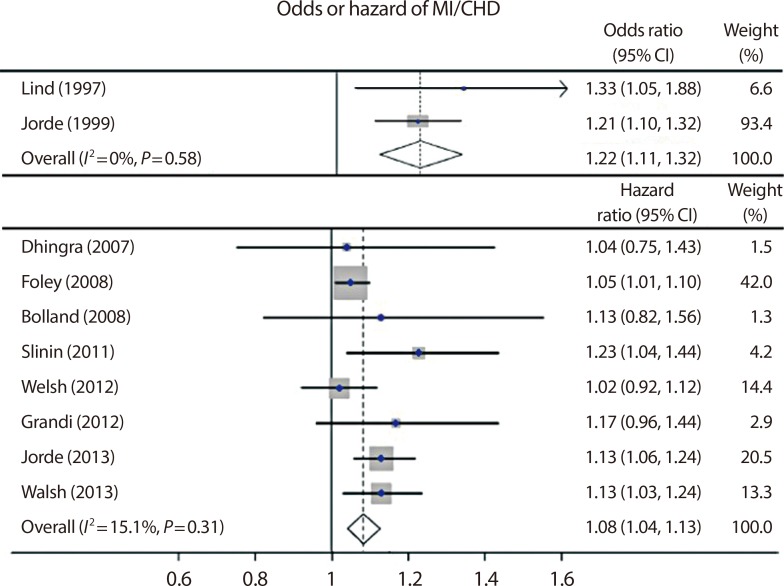 | Fig. 1Forest plots showing the relationships between serum calcium at baseline and subsequent cardiovascular events over a weighted mean follow-up period of 12.4 years. Only studies reporting a linear relationship are included. Data are shown separately for odds and hazard ratios, which are expressed per standard deviation of serum calcium. 95% confidence intervals (CIs) are shown. The result of each meta-analysis is shown as a diamond. Adapted from Reid et al., with permission from John Wiley and Sons [1]. MI, myocardial infarction; CHD, coronary heart disease.
|
Go to :
MECHANISMS OF THE CALCIUM-VASCULAR DISEASE CONNECTION
The association of serum calcium with subsequent vascular disease events and mortality raises the question as to whether calcium levels have a causative role in this association. The simplest scenario would be to postulate that circulating calcium levels directly promote vascular calcification, and there are two very large studies (total patient population >30,000) from Korea showing that coronary artery calcification is directly related to circulating calcium levels [67]. Like the data on cardiovascular events, these associations are attenuated but not removed by adjustment for blood pressure, BMI, and other vascular risk factors. Other studies have shown associations of serum calcium with aortic calcification [8] and carotid artery plaque [910]. The attenuation of the association following adjustment for vascular risk factors is consistent with other evidence that serum calcium is directly related to circulating lipids, glucose metabolism, BMI, and blood pressure (recently reviewed elsewhere) [1]. These risk factors could be intermediaries in a chain of causation or they could be independent associations not directly involved in the calcium-vascular link. Several lines of evidence potentially inform this discussion. Primary hyperparathyroidism is thought to be associated with increased vascular risk and is also associated with increased body weight and other metabolic disturbances. Surgical cure of this condition may improve blood pressure, endothelial dysfunction, echocardiographic changes, and metabolic abnormalities, but results are inconsistent with both positive [11121314151617] and negative [11181920] findings. It is notable; however, that genetic variations of the calcium-sensing receptor which increase serum calcium by about 0.025 mmol/L are associated with an odds ratio for coronary heart disease (CHD) of 1.25 and an odds ratio for cardiovascular mortality of 1.48 [21]. In this context, it is clear that the primary abnormality is the serum calcium. Complementing this, is clinical trial evidence that reducing serum calcium with the use of EDTA reduces cardiovascular event rates by 18% [22]. There is direct experimental evidence that raising serum calcium raises blood pressure [2324], possibly mediated by changes in intracellular calcium which regulates vascular smooth muscle contraction. These changes might account for the higher blood pressures, compared with controls, observed following acute ingestion of calcium supplements [2526]. A randomised controlled trial (RCT) of a calcium-fortified milk over 2 years, demonstrated an increase in aortic calcification in those randomised to the milk [27], calcium supplements increased carotid intima-media thickness in a RCT of postmenopausal women [28], and calcium supplement use is associated with increased risk of developing coronary artery calcification [29].
Direct vascular effects are not the only possibility to be considered. Calcium is intimately involved in the coagulation pathway and also regulates platelet function via the calcium-sensing receptor [30]. Hypercalcaemia in rats accelerates clot initiation [31] and in human blood samples ionised calcium is associated with clot initiation and clot strength [32]. The increased platelet activation of patients with primary hyperparathyroidism also suggests that circulating calcium regulates coagulation in vivo [33] and this is further supported by increases in blood coagulability 4 hours after an oral calcium load in normal postmenopausal women [25].
Go to :
CALCIUM SUPPLEMENTS INCREASE CIRCULATING CALCIUM
The findings discussed above suggest that circulating calcium probably does play a pathogenic role in development of cardiovascular disease. This raises the question of whether dietary calcium intake or the use of calcium supplements influences vascular health. It is common practice to assess serum calcium in the fasting state and conclude that both diet and supplement use do not influence circulating calcium concentrations. However, studies immediately following calcium ingestion paint a different picture showing increases in total calcium of 0.05 to 0.15 mmol/L, depending on the source of calcium and the amounts administered. Fig. 2 compares the calcaemic effects of a dairy-rich meal with those of a calcium citrate supplement, demonstrating higher and more sustained calcaemic effects from the supplement [34]. If the supplement was taken after a meal, its calcaemic effects were not attenuated, but they did appear to be prolonged (Fig. 2B). In this study, calcium in the form of a fortified orange juice had much the same profile as a supplement. Some of the largest calcium increments have been found with fortified dairy products which can elevate total calcium by 0.15 mmol/L and sustain this increment for >5 hours [35].
 | Fig. 2Effects of calcium supplements on serum total calcium concentration in normal postmenopausal women. (A) The calcaemic effects of calcium (500 mg) as citrate administered fasting (closed circles) are contrasted with those of a dairy product meal with the same calcium content. (B) The calcaemic effects of calcium (500 mg) as citrate are contrasted when administered fasting (closed circles) or with a meal (open circles). (C) The calcaemic effects of 1 g calcium as citrate is shown at baseline in calcium-naive women (closed circles) or after 3 months of daily use of a 1 g calcium supplement (open circles). Adapted from Bristow et al., with permission from Cambridge University Press [3436]. aSignificantly different from citrate-fasting (P<0.05).
|
Some writers have dismissed these excursions in serum calcium as having no biological significance. However, the associations between vascular events and mortality with variations in serum calcium within the normal range, make clear that differences of 0.05 to 0.1 mmol/L are indeed associated with clinically important endpoints. In the longitudinal studies relating serum calcium to vascular risk, it is assumed that the differences between individuals and serum calcium are sustained over time. Changes following food ingestion or calcium supplementation are transient, but do last for at least 6 to 8 hours, and are likely to be repeated each time a supplement is ingested. Indeed, we have shown that the excursion in serum calcium after a 1 g dose of calcium is at least as large in long-term users of supplements as it is in calcium-naive subjects (Fig. 2C) [36].
Go to :
TRIALS OF CALCIUM SUPPLEMENTS IN PATIENTS WITH RENAL IMPAIRMENT
The area of medical practice in which concern about the cardiovascular safety of calcium supplements has been enunciated for the longest is that of renal medicine. Hyperphosphataemia is present long before the need for dialysis arises, and this has been managed with a succession of phosphate-binding agents, including calcium supplements. Vascular calcification is evident on plain radiographs in many patients with renal failure and concern has been expressed that the use of calcium supplements might accelerate this phenomenon, resulting in even higher incidences of vascular events. As a result of these concerns, phosphate binders that do not contain calcium have also been developed and a series of trials carried out comparing mortality following the use of these agents. These studies have recently been meta-analysed with the finding that mortality is 20% lower in individuals using calcium-free binders [37]. It is important to note that two trials have been carried out in patients not yet requiring dialysis. In the first of these, Russo et al. [38] showed that calcium supplements increased coronary artery calcification when compared with sevelamer, a calcium-free phosphate binder. Subsequently, Di Iorio et al. [39] showed that mortality was 10% in sevelamer-treated patients with stage three or four chronic renal failure (mean baseline creatinine clearance 33 mL/min) but rose to 19% in those randomised to calcium. This is a finding of broad relevance, since many older patients who might consider taking calcium supplements for treatment or prevention of osteoporosis, have creatinine clearances in this range.
Go to :
TRIALS OF CALCIUM SUPPLEMENTS IN OTHER POPULATIONS
Publication of the cardiovascular findings from the Auckland Calcium Study broadened the focus of concern regarding safety of calcium supplements to the entire adult population. This study in 1,471 healthy postmenopausal women primarily addressed efficacy in osteoporosis prevention, but did pre-specify cardiovascular endpoints as secondary efficacy outcomes, the hypothesis being that a benefit might be found. It was a surprise; therefore, to observe a significant excess of myocardial infarctions in those randomised to calcium, something not previously reported in individuals without renal disease [40]. This led Bolland et al. [41] to seek unpublished cardiovascular event data from all major calcium studies up to that time, which he published in 2010, reporting the relative risk of myocardial infarction of 1.27 (95% CI, 1.01 to 1.59) and a smaller adverse effect on stroke (relative risk, 1.12; 95% CI, 0.92 to 1.36).
At that time, the other substantial body of data addressing this question came from the Women's Health Initiative (WHI), in which 36,000 postmenopausal women were randomised to placebo or to an intervention consisting of calcium+vitamin D. This study had reported a HR for a combined endpoint of myocardial infarction or CHD death of 1.04 (95% CI, 0.92 to 1.18), and for a broader endpoint that also included coronary revascularisation, a HR of 1.08 (95% CI, 0.99 to 1.19) [42]. There was an interaction of the treatment effect on myocardial infarction or CHD death with BMI, such that the adverse effect was greater in the non-obese, with a HR of 1.17. The investigators concluded that there was no proof of adverse cardiovascular effect, but in the broader context of the other information available at that time these data cannot be regarded as entirely reassuring.
The apparent discrepancy between the Bolland meta-analysis of calcium supplements and the findings from the WHI could be attributed to the addition of vitamin D in the latter study, the younger age of the WHI cohort, or to the widespread self-administration of calcium supplements at randomisation (54%) and subsequently (69% at study end) in the WHI. We, therefore, submitted a proposal (to the National Institutes of Health who held the WHI data) for an analysis to determine whether the use of calcium supplements at the time of randomisation influenced the effects of the calcium+vitamin D intervention on cardiovascular risk. A significant interaction was found, such that myocardial infarction increased 22% in those who were calcium-naive, but there was no evidence of an adverse effect in those already taking calcium supplements at the time of randomisation [43]. These findings were incorporated into a second meta-analysis which looked at trials of calcium alone or calcium+vitamin D and found the risk of myocardial infarction was increased about 25%, with a 15% increase in stroke risk, the latter of borderline statistical significance. The extent to which the WHI data from calcium-naive subjects recapitulates what was found in the Bolland meta-analysis of calcium supplements is striking. Not only are the sizes of the effects the same, but the different time-courses of the effects of calcium on myocardial infarction and stroke are also reproduced (Fig. 3) [44]. However, the absence of an adverse effect of adding a further supplement to those already taking calcium indicates that the effect of calcium is not dose-dependent. An insight into the reason for this is provided by the data shown in Fig. 2, where a doubling in calcium dose has a barely discernible effect on the size of the increase in serum calcium that results. This is consistent with the failure of an increased dose of calcium supplement to influence vascular risk in the WHI participants already receiving supplements.
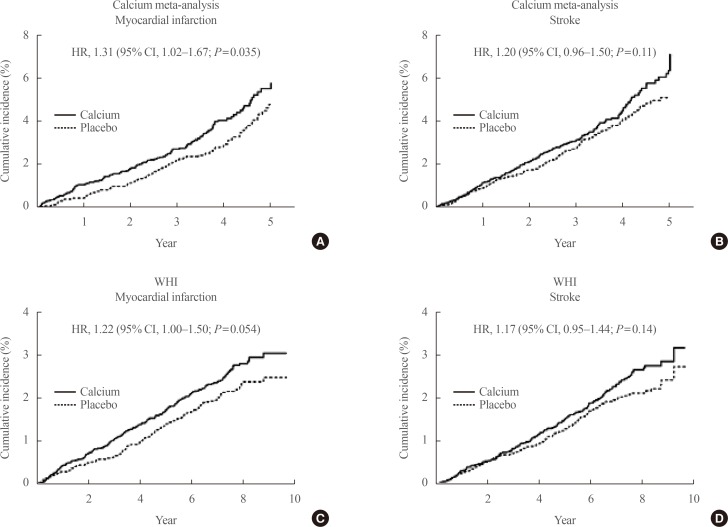 | Fig. 3Kaplan-Meier survival curves for time to incident myocardial infarction or stroke by treatment allocation in a meta-analysis of patient-level data from five trials of calcium supplements used as monotherapy (n=8,151) (A, B), and calcium-naive women in the Women's Health Initiative (WHI) calcium and vitamin D trial (n=16,718) (C, D). The magnitude and time-course of the effects of calcium supplements on the two groups of vascular events were very similar in these independent databases. Adapted from Radford et al. [44]. HR, hazard ratio; CI, confidence interval.
|
The results of these meta-analyses and those of a much smaller study from Wang are summarised in the Table 1 [4143454647484950]. Several further meta-analyses have followed, with a variety of results which is bewildering to anyone not intimately familiar with these data. The other meta-analyses are also shown in the Table 1 together with comments regarding the methodological differences that have resulted in divergent outcomes. The differences arise because of the use of different endpoints (myocardial infarction versus much broader definitions of vascular disease) and the inclusion of different study populations. For example, the Lewis meta-analysis chose to ignore the interaction between baseline calcium supplement use and the effect of calcium+vitamin D on myocardial infarction in the WHI, and so included the entire WHI cohort [45]. The WHI participants contributed 82% of the weight of this analysis, which therefore is effectively a re-publication of the WHI data reported earlier by Hsia et al. [42]. They also included the Larsen study [51], which was a cluster-randomised study with only one cluster per intervention and non-comparability of the treatment groups. Thus, its inclusion is inappropriate. Most recently, Chung et al. [52] published “Calcium intake and cardiovascular disease risk: an updated systematic review and meta-analysis” of these data, which did not include a meta-analysis of the RCTs. Overlooking much of the available data shown in the Table 1, they concluded there were inadequate RCTs for meta-analysis. Their review of this area, has other methodological problems, discussed elsewhere [53].

Table 1
Meta-Analyses of RCTs of Effects of Calcium Supplements on Cardiovascular Events
| Study | Intervention | No. | Endpoint (s) | Findings | Comments |
|---|---|---|---|---|---|
| Wang et al. (2010) [46] | Calcium | 3,861 | CVD | RR, 1.14 (0.92–1.41) | Trial level analysis of 3 published studies |
| Bolland et al. (2010) [41] | Calcium | 11,921 | MI | RR, 1.27 (1.01–1.59) | 11 Studies, including previously unpublished data; 23% of MIs were self-reported: exclusion of these raises RR to 1.44 (1.08–1.91) [47] |
| Stroke | RR, 1.12 (0.92–1.36) | ||||
| Bolland et al. (2011) [43] | Calcium±D | 28,072 | MI | RR, 1.24 (1.07–1.45) | WHI data is from women who were not already taking calcium supplements at randomization; 9% of MIs self-reported: exclusion of these raises RR to 1.29 (1.10–1.52) |
| Stroke | RR, 1.15 (1.00–1.32) | ||||
| Wang et al. (2012) [50] | Calcium | 3,861 | CV events | RR, 1.14 (0.92–1.41) | Trial level analysis of 3 published studies |
| Calcium+D | 37,653 | RR, 0.99 (0.79–1.22) | Included WHI women already taking calcium. WHI dominates outcome | ||
| Mao et al. (2013) [48] | Calcium | ~7,454 | MI | OR, 1.28 (0.97–1.28) | - |
| Stroke | OR, 1.14 (0.90–1.46) | ||||
| Calcium±D | ~39,609 | MI | OR, 1.06 (0.92–1.21) | Included WHI women already taking calcium. WHI dominates outcome | |
| Lewis et al. (2015) [45] | Calcium | 6,333 | MI | RR, 1.37 (0.98–1.32) | Excluded men and self-reported events |
| Calcium±D | 48,460 | CHD | RR, 1.02 (0.96–1.09) | Included 4 RCTs and the non-RCT of Larsen. WHI women already taking calcium included; 82% weight from WHI [49]. |
RR and OR are shown with 95% confidence intervals.
RCT, randomized controlled trial; CVD, cardiovascular disease; RR, relative risk; MI, myocardial infarction; Calcium±D, calcium with or without vitamin D; WHI, Women's Health Initiative; CV, cardiovascular; OR, odds ratio; CHD, coronary heart disease.
![]()
The findings in the Table 1 can be summarised as follows: there is a consistent adverse trend in risk of myocardial infarction and, less so, for stroke, across individual trials, and their meta-analyses. Second, this adverse trend is not apparent when a much broader cardiovascular endpoint is used. Third, when considering trials using a combined calcium/vitamin D intervention, the data from other studies are swamped by that from the WHI, and the outcome of the meta-analysis is determined by whether the highly influential effect of baseline calcium use on the outcomes of that study is considered.
Thus, interpretation of these data hinges on which WHI analysis is used. Do we consider the calcium-naive subjects in whom there is a significant increase in risk of myocardial infarction of exactly the same magnitude as is seen in the other studies, or do we place the emphasis on the larger number of individuals already taking calcium supplements at randomisation. Certainly, the convention for understanding the effects, beneficial or adverse, of interventions is to trial their use in individuals not already receiving that intervention. This suggests that the data in the calcium-naive subjects should guide decision-making.
In their totality, these data raise significant concerns regarding the cardiovascular safety of calcium supplements, similar to those found with other osteoporosis medicines which have been discontinued recently (e.g., strontium and odanacatib) [54]. The parallel with strontium is particularly relevant, since that agent belongs to the same group of elements in the periodic table as calcium, binds to the calcium-sensing receptor, and can substitute for calcium in many of its biological activities.
Go to :
EFFECTS OF DIETARY CALCIUM ON CARDIOVASCULAR RISK
There has been a large number of observational studies of the influence of dietary calcium intake on cardiovascular risk. The results of these cover most conceivable outcomes and are, therefore, generally unhelpful. Meta-analysis of these studies has produced a relative risk of cardiovascular mortality of 0.97 (95% CI, 0.89 to 1.07) comparing the highest and lowest calcium intake groups. However, more detailed analysis suggested a U-shaped association between dietary calcium intake and cardiovascular mortality, with lowest mortality at about 800 mg/day [55].
A problem with observational studies is confounding by other dietary and lifestyle variables. In countries where calcium has been promoted as an important contributor to bone health, more health-conscious and motivated individuals will tend to have higher calcium intakes, but this might not be the cause of their better medical outcomes. Also, the source of high dietary calcium intakes will vary from country to country, but they will commonly be produced by high intakes of dairy products. If this is in the form of full-cream milk, then this may provide a substantial a load of saturated fats which will produce an adverse effect. However, if the dairy product intake is predominantly low-fat cheeses, then the cardiovascular effects could be quite different. The general consensus from these conflicting data is that there is currently no good evidence to support limiting dietary calcium intake for reasons of cardiovascular safety.
The apparent difference between dietary calcium intake and calcium supplement use on vascular risk is consistent with their different effects on blood calcium levels. As Fig. 2 demonstrates, there is no reduction in the calcaemic effect of a calcium supplement over time. In contrast, a sustained high dietary calcium intake results in reduced efficiency of intestinal absorption and increased urinary calcium excretion, so that the long-term effect of dietary calcium on blood calcium and bone density is negligible [56]. The failure of the calcaemic effect of calcium supplements to diminish with long-term use, suggests that this is not mediated by the regulated, active absorption mechanism in the upper gastrointestinal tract, but by the unregulated, paracellular absorption route.
Go to :
ROLE OF CALCIUM IN BONE HEALTH
When providing advice regarding calcium intake to individuals and populations, the potential benefits and risks of calcium need to be considered. While there is little evidence that dietary calcium intakes above 500 mg/day influence postmenopausal bone loss [57], bone density [56], or fracture risk [58], there is no compelling evidence that high intakes carry significant risk, except in those with a history of renal calculi. The balance of risks and benefits for calcium supplements is rather different, with significant evidence suggesting an adverse cardiovascular effect, and strong evidence of increased risk of renal calculi [59] and of gastrointestinal side-effects [60], sometimes severe. Therefore, advocating use of supplements, except in those with very low calcium intakes (e.g., those on calcium-free diets), seems to have little merit. The fact that supplements do not produce cumulative benefits on bone density [56] and that studies in community-dwelling individuals show no benefit on fracture [58], suggest there is no case made for their use to prevent osteoporosis. The limited evidence available suggests that in osteoporosis treatment, pharmaceutical interventions are as effective in those using supplements as in those who are not [61]. Therefore, supplementation with calcium should not be routine in osteoporosis. The dietary and lifestyle advice given to people at risk of osteoporosis should focus on maintenance of BMI above 20, regular exercise for falls prevention, safety in the home, and smoking cessation. Timely assessment of fracture risk, and institution of pharmaceutical interventions in those at elevated risk are also critical to the prevention of fractures in older women and men.
Go to :
CONCLUSIONS
Circulating calcium is a risk factor for vascular disease, though the precise underlying mechanisms remain to be confirmed. This conclusion is based on large observational cohorts and on Mendelian randomization studies [62]. This finding is relevant to the use of calcium supplements, since these agents increase serum calcium levels for some hours after each ingestion, by an amount that is associated with a clinically relevant increase in risk in the observational studies. In chronic kidney disease patients, trial data indicate increased cardiovascular risk associated with calcium supplement use, so most physicians now use other forms of phosphate binders. In osteoporosis management there is ongoing controversy, though meta-analyses of trial data raise real concern that these supplements carry more risk than benefit. In community-dwelling populations, the balance of evidence indicates that calcium nutrition is not a critical contributor to bone health and that fracture prevention strategies should focus on weight maintenance, falls prevention and timely introduction of pharmaceuticals to increase bone mass.
Go to :
 XML Download
XML Download