This article has been
cited by other articles in ScienceCentral.
Abstract
The prevalence of hypercholesterolemia in Koreans 30 years old and over was 19.5% in 2015 according to the Korean Nutrition and Health Examination Survey, which means that one-fifth of adults had hypercholesterolemia. The prevalence of hypertriglyceridemia in adults 30 years of age and older was 16.8% in 2015, and men had a 2-fold higher prevalence of hypertriglyceridemia than women (23.9% vs. 10.4%). The awareness of hypercholesterolemia in Koreans was higher in women than among men (62.4% vs. 51.4%). It increased with age; the level of awareness in participants 30 to 49 years of age (32.1% in men and 32.6% in women) was less than half of that observed among respondents ≥65 years old (77.5% in men and 78.0% in women). Regular check-ups for dyslipidemia and the active management thereof are urgent in Korean men aged 30 to 49. In women, the perimenopausal period is crucial for the prevention and management of metabolic syndrome, including dyslipidemia. Overall, improvements in awareness and treatment in the age group of 30 to 49 years in both men and women remain necessary.
Go to :

Keywords: Dyslipidemias, Hypercholesterolemia, Hypertriglyceridemia, Metabolic syndrome
INTRODUCTION
Dyslipidemia is a leading cause of cardiovascular disease and mortality worldwide [
12]. According to data from Statistics Korea [
3], the leading cause of death was cancer in 2015, with the second and third ranks occupied by heart disease and cerebrovascular disease, respectively. Diabetes was the sixth most common cause of death. Atherosclerosis is a preceding pathologic condition in the development of both heart and cerebrovascular diseases [
45], and dyslipidemia is the greatest risk factor for atherosclerosis. Therefore, there is no doubt that dyslipidemia is a major risk factor for cardiovascular disease and mortality in Koreans. This review article will discuss the epidemiologic characteristics of dyslipidemia in Korean adults. The statistics regarding the prevalence of dyslipidemia in Korean adults in this article were obtained from the Korean Nutrition and Health Examination Survey (KNHANES) conducted from 2010 to 2015 [
6].
Go to :
PREVALENCE OF HYPERCHOLESTEROLEMIA IN KOREANS
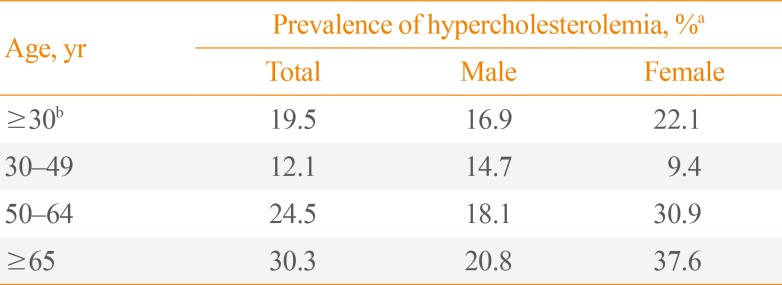
The prevalence of hypercholesterolemia in Koreans 30 years old and over was 19.5% in 2015 (
Table 1). Hypercholesterolemia was defined as a serum total cholesterol level ≥240 mg/dL or the use of lipid-lowering medications. The estimated population with hypercholesterolemia was approximately 6.6 million. The prevalence of hypercholesterolemia increased in an age-dependent manner; in particular, it increased approximately 3-fold in women in their 50s and older. Trends in the prevalence of hypercholesterolemia over the last 5 years are shown in
Table 2. It increased from 13.5% in 2010 to 17.9% in 2015. Moreover, it increased from 8.0% in 2005 to 13.5% in 2010; it then remained steady for the following 5 years, but increased by 3.3% points in 2015.
Table 1
Prevalence of Hypercholesterolemia among Korean Adults ≥30 Years Old in 2015
|
Age, yr |
Prevalence of hypercholesterolemia, %a
|
|
Total |
Male |
Female |
|
≥30b
|
19.5 |
16.9 |
22.1 |
|
30–49 |
12.1 |
14.7 |
9.4 |
|
50–64 |
24.5 |
18.1 |
30.9 |
|
≥65 |
30.3 |
20.8 |
37.6 |

Table 2
Trends in the Prevalence of Hypercholesterolemia, 2010 to 2015

|
Variable |
Hypertriglyceridemia, %a
|
|
2010 |
2011 |
2012 |
2013 |
2014 |
2015 |
|
Total |
13.5±0.6 |
13.8±0.5 |
14.5±0.6 |
14.9±0.6 |
14.6±0.7 |
17.9±0.7 |
|
Male |
13.0±0.9 |
12.6±0.9 |
12.2±0.8 |
13.6±0.8 |
13.9±1.0 |
16.5±1.0 |
|
Female |
13.4±0.7 |
14.9±0.7 |
16.4±0.9 |
15.9±0.8 |
15.0±0.8 |
19.1±0.8 |
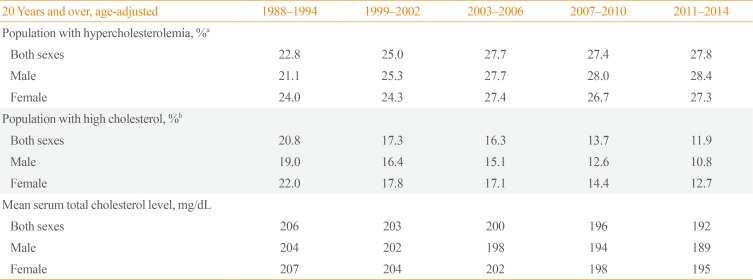
According to data from the National Health and Nutrition Examination Surveys (NHANES) in the United States [
7], the prevalence of hypercholesterolemia in adults aged 20 and over increased from 22.8% in the 1988 to 1994 surveys to 27.8% in the 2011 to 2014 surveys (
Table 3). Considering the difference in the age of the population between the KNHANES (30 and over) and NHANES (20 and over), its prevalence in the United States is quite high. However, the percent of the population with high cholesterol declined from 20.8% in the 1988 to 1994 surveys to 11.9% in the 2011 to 2014 surveys. The mean serum total cholesterol level also declined during the same period in the United States. This means that the increasing pattern of hypercholesterolemia in United States is mainly due to an increasing percentage of the population taking lipid-lowering medications [
8]. This corresponds to a decreasing pattern of cardiovascular diseases such as coronary heart disease [
910]. In contrast, the mean serum total cholesterol level did not decline in Korea during roughly the same period (from 183.9±0.64 mg/dL in 1998 to 185.1±0.64 mg/dL in 2010) [
11], even though the percentage of the population taking lipid-lowering medications increased over the past 10 years in Korea (from 2.8% in 2003 to 12.9% in 2013) [
12].
Table 3
Cholesterol Levels among Adults Aged 20 and over in the United States Based on the National Health and Nutrition Examination Survey for Selected Years (1988 to 1994 through 2011 to 2014)
|
20 Years and over, age-adjusted |
1988–1994 |
1999–2002 |
2003–2006 |
2007–2010 |
2011–2014 |
|
Population with hypercholesterolemia, %a
|
|
|
|
|
|
|
Both sexes |
22.8 |
25.0 |
27.7 |
27.4 |
27.8 |
|
Male |
21.1 |
25.3 |
27.7 |
28.0 |
28.4 |
|
Female |
24.0 |
24.3 |
27.4 |
26.7 |
27.3 |
|
Population with high cholesterol, %b
|
|
|
|
|
|
|
Both sexes |
20.8 |
17.3 |
16.3 |
13.7 |
11.9 |
|
Male |
19.0 |
16.4 |
15.1 |
12.6 |
10.8 |
|
Female |
22.0 |
17.8 |
17.1 |
14.4 |
12.7 |
|
Mean serum total cholesterol level, mg/dL |
|
|
|
|
|
|
Both sexes |
206 |
203 |
200 |
196 |
192 |
|
Male |
204 |
202 |
198 |
194 |
189 |
|
Female |
207 |
204 |
202 |
198 |
195 |
Go to :
PREVALENCE OF HYPERTRIGLYCERIDEMIA IN KOREANS
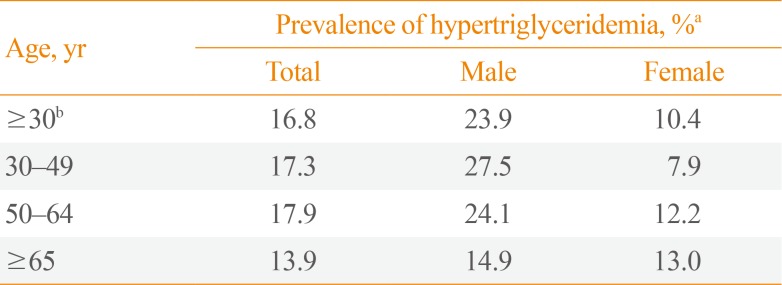
The prevalence of hypertriglyceridemia in adults aged 30 and over was 16.8% in 2015, and the estimated population with hypertriglyceridemia was approximately 5.8 million (
Table 4). Men had a 2-fold higher prevalence of hypertriglyceridemia than was observed in women (23.9% vs. 10.4%). Among participants under 50 years of age, this difference was much larger, with a 3-fold higher prevalence in men (27.5% vs. 7.9%). This means that one out of every three or four Korean men aged 30 to 49 has hypertriglyceridemia.
Table 4
Prevalence of Hypertriglyceridemia in Korean Adults ≥30 Years Old in 2015
|
Age, yr |
Prevalence of hypertriglyceridemia, %a
|
|
Total |
Male |
Female |
|
≥30b
|
16.8 |
23.9 |
10.4 |
|
30–49 |
17.3 |
27.5 |
7.9 |
|
50–64 |
17.9 |
24.1 |
12.2 |
|
≥65 |
13.9 |
14.9 |
13.0 |
Although little change was observed in the prevalence of hypertriglyceridemia in the most recent 5 years (from 16.6 % in 2010 to 16.8% in 2015), a large increase has taken place over the last 20 years, since the prevalence of hypertriglyceridemia in 1998 was only 10.2%, and a much lower level was also observed in men (14.9%) (
Table 5).
Table 5
Trends in the Prevalence of Hypertriglyceridemia, 2010 to 2015

|
Variable |
Hypertriglyceridemia, %a
|
|
2010 |
2011 |
2012 |
2013 |
2014 |
2015 |
|
Total |
16.6±0.7 |
16.2±0.7 |
16.8±0.8 |
17.1±0.7 |
17.9±0.8 |
16.8±0.8 |
|
Male |
23.9±1.3 |
23.9±1.2 |
21.1±1.3 |
23.8±1.3 |
26.8±1.3 |
24.6±1.5 |
|
Female |
9.7±0.7 |
8.9±0.7 |
12.5±0.9 |
10.9±0.7 |
9.8±0.8 |
9.7±0.8 |
Similar trends regarding sex and age differences in hypertriglyceridemia can be seen in the NHANES [
13]. Even though the definition for hypertriglyceridemia is different in the NHANES, where it is defined as a triglyceride level of 150 mg/dL or more, approximately one-fourth of adults aged 20 and over had hypertriglyceridemia in the 2009 to 2012 surveys. A sex difference was seen in adults aged 20 to 39 (25.1% in men vs. 14.7% in women) and 40 to 59 (34.9% in men vs. 23.0% women), but not in adults aged 60 and over. However, the prevalence of hypertriglyceridemia declined from 33.3% in the 2001 to 2004 surveys to 25.1% in the 2009 to 2012 surveys. This declining pattern was seen in both sexes and all age groups, unlike what was observed in Koreans [
11].
Although low density lipoprotein cholesterol is the primary target for lipid control in the prevention of cardiovascular diseases, high triglycerides combined with low levels of high density lipoprotein cholesterol is a typical profile of atherogenic dyslipidemia [
1415]. High triglycerides in males may occur due to alcohol consumption and unhealthy lifestyles in those age groups. For example, high-risk alcohol consumption, defined as an average consumption of ≥7 drinks in men (≥5 drinks in women) on ≥2 occasions per week was most common in males 30 to 49 years of age, and was 4- to 5-fold more common than in women of the same age group. Furthermore, the proportion of high-fat diets was approximately twice as high among men as among women in respondents 30 to 49 years of age (15.7% vs. 8.9%).
Therefore, active screening for hypertriglyceridemia and managing hypertriglyceridemia through lifestyle modifications, including reductions in alcohol consumption, are urgent and necessary for Korean men, especially those aged 30 to 49.
Go to :
MANAGEMENT OF HYPERCHOLESTEROLEMIA IN KOREANS
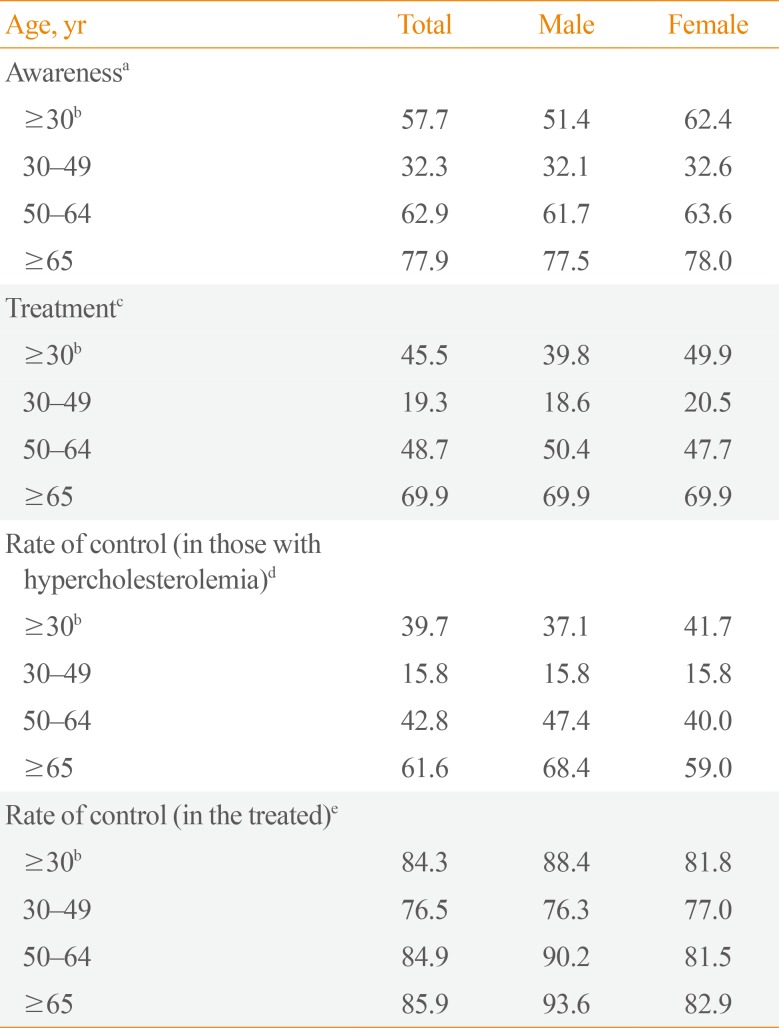
Awareness of hypercholesterolemia in Koreans was found to be greater among women than among men (62.4% vs. 51.4%) (
Table 6). It increased with age; the level of awareness in participants 30 to 49 years of age (32.1% in men and 32.6% in women) was less than half of that observed among respondents >65 years old (77.5% in men and 78.0% in women). Furthermore, the rate of treatment, which was defined as the proportion of the population taking a lipid-lowering medication ≥20 days a month, was only 45.5% in the population with hypercholesterolemia. Due to this unacceptably low rate of treatment, the rate of control in those with hypercholesterolemia, which was defined as the proportion of the population with hypercholesterolemia with a serum total cholesterol level <200 mg/dL, was also low, at 39.7%. However, the rate of control in the population treated with lipid-lowering medications was 84.3%, which means that when it is appropriately diagnosed and treated, hypercholesterolemia is easy to control.
Table 6
Management Status of Hypercholesterolemia in Participants of the Sixth Korean National Health and Nutrition Examination Survey (2013 to 2015)
|
Age, yr |
Total |
Male |
Female |
|
Awarenessa
|
|
|
|
|
≥30b
|
57.7 |
51.4 |
62.4 |
|
30–49 |
32.3 |
32.1 |
32.6 |
|
50–64 |
62.9 |
61.7 |
63.6 |
|
≥65 |
77.9 |
77.5 |
78.0 |
|
Treatmentc |
|
|
|
|
≥30b
|
45.5 |
39.8 |
49.9 |
|
30–49 |
19.3 |
18.6 |
20.5 |
|
50–64 |
48.7 |
50.4 |
47.7 |
|
≥65 |
69.9 |
69.9 |
69.9 |
|
Rate of control (in those with hypercholesterolemia)d
|
|
|
|
|
≥30b
|
39.7 |
37.1 |
41.7 |
|
30–49 |
15.8 |
15.8 |
15.8 |
|
50–64 |
42.8 |
47.4 |
40.0 |
|
≥65 |
61.6 |
68.4 |
59.0 |
|
Rate of control (in the treated)e
|
|
|
|
|
≥30b
|
84.3 |
88.4 |
81.8 |
|
30–49 |
76.5 |
76.3 |
77.0 |
|
50–64 |
84.9 |
90.2 |
81.5 |
|
≥65 |
85.9 |
93.6 |
82.9 |
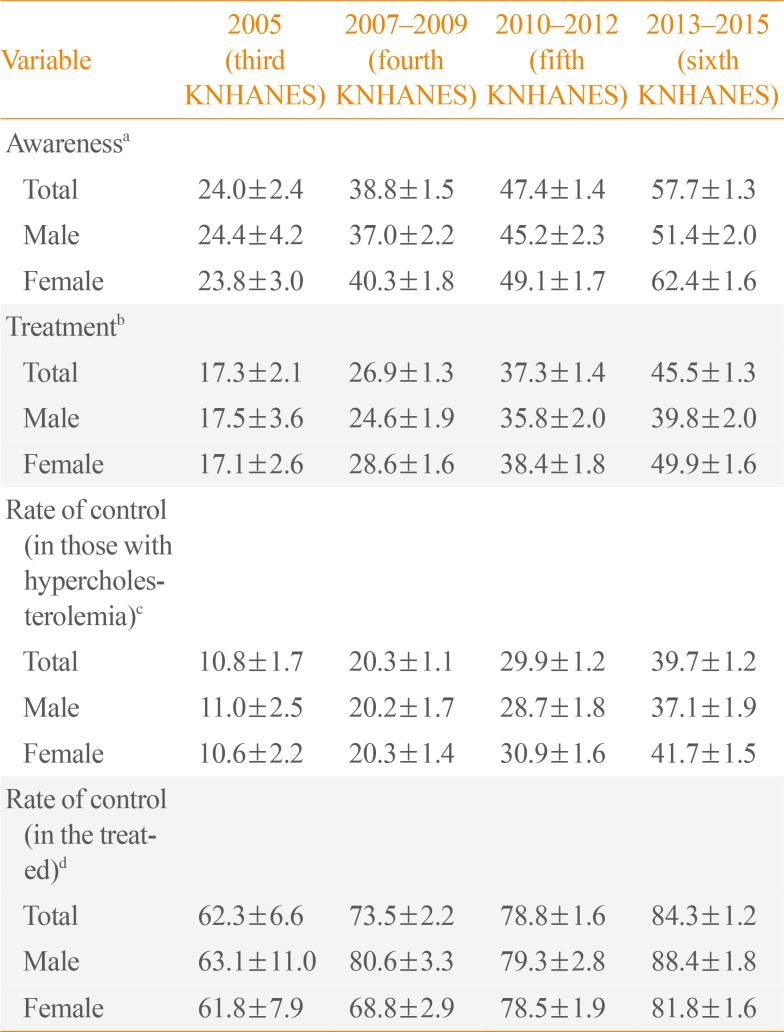
Table 7 shows the management status of hypercholesterolemia during the most recent 10 years; the awareness rate in 2005 was only 24.0%, and the treatment rate was 17.3%. Since then, through the fourth to sixth stages of the KNHANES, the rate of awareness and treatment has increased by 10% points at every stage. Thus, all parameters regarding management have improved by 20% to 30% points compared with those of the third KNHANES conducted in 2005.
Table 7
Management Status of Hypercholesterolemia during the Most Recent 10 Years
|
Variable |
2005 (third KNHANES) |
2007–2009 (fourth KNHANES) |
2010–2012 (fifth KNHANES) |
2013–2015 (sixth KNHANES) |
|
Awarenessa
|
|
|
|
|
|
Total |
24.0±2.4 |
38.8±1.5 |
47.4±1.4 |
57.7±1.3 |
|
Male |
24.4±4.2 |
37.0±2.2 |
45.2±2.3 |
51.4±2.0 |
|
Female |
23.8±3.0 |
40.3±1.8 |
49.1±1.7 |
62.4±1.6 |
|
Treatmentb
|
|
|
|
|
|
Total |
17.3±2.1 |
26.9±1.3 |
37.3±1.4 |
45.5±1.3 |
|
Male |
17.5±3.6 |
24.6±1.9 |
35.8±2.0 |
39.8±2.0 |
|
Female |
17.1±2.6 |
28.6±1.6 |
38.4±1.8 |
49.9±1.6 |
|
Rate of control (in those with hypercholesterolemia)c
|
|
|
|
|
|
Total |
10.8±1.7 |
20.3±1.1 |
29.9±1.2 |
39.7±1.2 |
|
Male |
11.0±2.5 |
20.2±1.7 |
28.7±1.8 |
37.1±1.9 |
|
Female |
10.6±2.2 |
20.3±1.4 |
30.9±1.6 |
41.7±1.5 |
|
Rate of control (in the treated)d
|
|
|
|
|
|
Total |
62.3±6.6 |
73.5±2.2 |
78.8±1.6 |
84.3±1.2 |
|
Male |
63.1±11.0 |
80.6±3.3 |
79.3±2.8 |
88.4±1.8 |
|
Female |
61.8±7.9 |
68.8±2.9 |
78.5±1.9 |
81.8±1.6 |
A recent study reported 30-year trends in mortality from cardiovascular diseases in Korea [
16]. The total cardiovascular disease mortality rate declined over the 30-year period from 1983 to 2012, but the mortality rate due to ischemic heart disease continuously increased. As discussed above, the prevalence of hypercholesterolemia has increased in both the United States and Korea, but with different underlying patterns. Therefore, to reduce the burden of cardiovascular disease in Korea, increasing the rate of treatment among those with hypercholesterolemia is essential.
Go to :
CONCLUSIONS
The prevalence of hypercholesterolemia in Koreans 30 years old and over was 19.5% in 2015, meaning that one-fifth of adults had hypercholesterolemia. Although the management of hypercholesterolemia has improved over the most recent 10 years, this improvement has not proven sufficient to reduce the burden of cardiovascular disease, so it remains necessary to improve awareness and treatment among adults aged 30 to 49. For hypertriglyceridemia, regular check-ups and active management are urgent in Korean men aged 30 to 49. For women, active screening in the perimenopausal period with the goal of preventing hypercholesterolemia and metabolic syndrome is very important.
Go to :
ACKNOWLEDGMENTS
This research was supported by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (NRF-2012R1A1A2007098).
Go to :
Notes
Go to :
References
1. Musunuru K. Atherogenic dyslipidemia: cardiovascular risk and dietary intervention. Lipids. 2010; 45:907–914. PMID:
20524075.

2. Haffner SM. Diabetes, hyperlipidemia, and coronary artery disease. Am J Cardiol. 1999; 83(9B):17F–21F.
3. Statistics Korea. Annual report on the causes of death statistics, 2015 [Internet]. Daejeon: Statistics Korea;c1996. cited 2017 Mar 5. Available from:
http://www.kostat.go.kr.
4. Libby P. Inflammation in atherosclerosis. Nature. 2002; 420:868–874. PMID:
12490960.
5. Reina SA, Llabre MM, Allison MA, Wilkins JT, Mendez AJ, Arnan MK, et al. HDL cholesterol and stroke risk: the Multi-Ethnic Study of Atherosclerosis. Atherosclerosis. 2015; 243:314–319. PMID:
26425994.
6. Ministry of Health and Welfare, Korea Centers for Disease Control and Prevention. Korea Health Statistics 2015: Korea National Health and Nutrition Examination Survey (KNHANES VI-3) [Internet]. Cheongju: Korea Centers for Disease Control and Prevention;2015. cited 2017 Mar 5. Available from:
http://knhanes.cdc.go.kr.
7. Centers for Disease Control and Prevention. Health, United States, 2015: Table 55. Cholesterol among adults aged 20 and over, by selected characteristics: United States, selected years 1988-1994 through 2011-2014. Atlanta: Centers for Disease Control and Prevention;2016. cited 2017 Mar 5. Available from:
http://www.cdc.gov/nchs/hus/contents2015.htm#055.
8. Gu Q, Paulose-Ram R, Burt VL, Kit BK. Prescription cholesterol lowering medication use in adults aged 40 and over: United States, 2003-2012. NCHS data brief, no 177. Hyattsville: National Center for Health Statistics;2014.
9. Sidney S, Quesenberry CP Jr, Jaffe MG, Sorel M, Nguyen-Huynh MN, Kushi LH, et al. Recent trends in cardiovascular mortality in the United States and public health goals. JAMA Cardiol. 2016; 1:594–599. PMID:
27438477.
10. Benjamin EJ, Blaha MJ, Chiuve SE, Cushman M, Das SR, Deo R, et al. Heart disease and stroke statistics 2017 update: a report from the American Heart Association. Circulation. 2017; 135:e146–e603. PMID:
28122885.
11. Roh E, Ko SH, Kwon HS, Kim NH, Kim JH, Kim CS, et al. Prevalence and management of dyslipidemia in Korea: Korea National Health and Nutrition Examination Survey during 1998 to 2010. Diabetes Metab J. 2013; 37:433–449. PMID:
24404515.
12. Korean Society of Lipidology and Atherosclerosis Dyslipidemia. Dyslipidemia fact sheet in Korea 2015 [Internet]. Seoul: Korean Society of Lipidology and Atherosclerosis Dyslipidemia;2017. cited 2017 Mar 5. Available from:
http://www.lipid.or.kr.
13. Carroll MD, Kit BK, Lacher DA. Trends in elevated triglyceride in adults: United States, 2001-2012. NCHS data brief, no 198. Hyattsville: National Center for Health Statistics;2015.
14. Austin MA, Hokanson JE, Edwards KL. Hypertriglyceridemia as a cardiovascular risk factor. Am J Cardiol. 1998; 81:7B–12B. PMID:
9462597.
15. Nordestgaard BG, Varbo A. Triglycerides and cardiovascular disease. Lancet. 2014; 384:626–635. PMID:
25131982.
16. Lee SW, Kim HC, Lee HS, Suh I. Thirty-year trends in mortality from cerebrovascular diseases in Korea. Korean Circ J. 2016; 46:507–514. PMID:
27482259.
Go to :


 PDF
PDF ePub
ePub Citation
Citation Print
Print



 XML Download
XML Download