

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
With dietary modification being a cornerstone of the management of diabetes, physicians must be ready to deal with peculiar dietary choices when managing patients with diabetes. An example of such patients is Muslim patients wishing to fast Ramadan, the 9th lunar month. The religious Ramadan fast entails abstaining from food and drink from dawn till sunset. Traditionally, Muslims break their fast with a meal at sunset (also called Iftar), followed by a second meal before dawn (Suhur), with variable snacks during the course of the night [1]. Although chronic illness exempts Muslims from this fast (Quran 2:183–185), many patients with diabetes choose to fast [2] in face of the possible adverse effects to their health, including hypoglycemia, diabetic ketoacidosis (DKA), and non-ketotic hyperosmolar state (NKHS) [2], in addition to dehydration, thrombosis, stroke, and retinal artery occlusion [3].
Nevertheless, the choice to fast remains a personal one, necessitating the study of safe diabetes management during Ramadan. The consensus favors the individualization of treatment [4567 8], with certain clinical trials providing more details for specific anti-diabetic drug therapies [910111213]. However, clinical data with regard to the safety of multi-drug regimens during fasting are particularly scarce, with the majority focusing on dual drug therapies and comparing only two-drug-regimens. To the best of the authors' knowledge, the only study to compare more than two drugs during Ramadan included three drugs; glimepiride, repaglinide, and insulin glargine and included 49 type 2 diabetes mellitus (T2DM) patients and 16 controls [14]. The aim of this study was to assess the safety of a protocol involving dose adjustments to four different anti-diabetic drug regimens in T2DM patients who chose to fast during Ramadan. These regimens included five drugs: sulfonylureas, metformin, insulin glargine, regular insulin and premixed insulin 70/30 (30% regular insulin and 70% isophane insulin), which are among the most commonly used and widely accessible management options for T2DM.
METHODS
Study design and patient selection
This prospective, observational, open-label study was conducted at the Endocrinology and Diabetes Clinics at Jordan University Hospital (JUH), Amman, Jordan, and spanned the month of Ramadan and the preceding month (from May 28, 2014 to July 27, 2014). The study was approved by the Institutional Review Board of the hospital and was carried out in accordance to the Ethical Principles for Medical Research Involving Human Subjects outlined in the Declaration of Helsinki. Written forms of consent were acquired from all of the participating patients.
A total of 468 patients were enrolled at the start of the study. Volunteers were sought among the Muslim T2DM patients attending the Endocrinology and Diabetes Clinics for their regular visits, with no incentives rewarded. As a criterion for enrollment, patients had to be consenting adults with a baseline glycated hemoglobin (HbA1c) value greater than 6.5% (48 mmol/mol) and less than 10% (86 mmol/mol). To avoid serum glucose fluctuations, only those who had been on a constant anti-diabetic drug regimen for at least 3 months before the study period were included.
Patients with any degree of cognitive dysfunction that might have impaired their capacity to provide consent were excluded, as were those older than 75 years, in whom the complications of poor glycemic control were deemed too dangerous. Additionally, female patients of reproductive age were excluded because females are exempted from fasting during their menstrual periods. Other causes of ineligibility included pregnant females up to 6 weeks postpartum; lactating females; patients with hypoglycemic unawareness, liver cirrhosis, renal impairment (defined as serum creatinine ≥1.5 mg/dL and/or an estimated creatinine clearance <40 mL/min/1.72 m2), or unstable seizure disorder; and patients with a history of depression, bipolar disorder, psychosis, or recurrent severe hypoglycemic attacks. Patients with recent histories of niacin or steroid therapy (within the month prior to the trial) or DKA or NKHS (within 3 months prior to the trial) were also excluded. Finally, patients living alone were excluded because those patients are less likely to receive rapid assistance if complications were to occur.
At least 2 weeks before the study period, the eligible patients were asked to come in for a screening visit, during which appropriate medical counseling was provided orally by the same physician regarding the risks of fasting and the need to modify treatment regimens during Ramadan. Guidance was also provided as to the importance of complying with the treatment, consuming meals regularly, identifying and treating hypoglycemia, and breaking the fast immediately whenever the patients' health required it, including hypoglycemia. No modifications to the patients' baseline exercise or dietary habits were made so that they could continue the study period as normally as they would to better mimic real life. A detailed patient history was then taken, and a thorough physical exam was performed, after which a blood sample was drawn for the following tests: serum creatinine, electrolytes, liver function, fasting lipid profile, complete blood count, glucose, and HbA1c. For these tests, blood samples were drawn from the fasting patients by trained medical residents at the clinic and were immediately sent to the local laboratory at JUH.
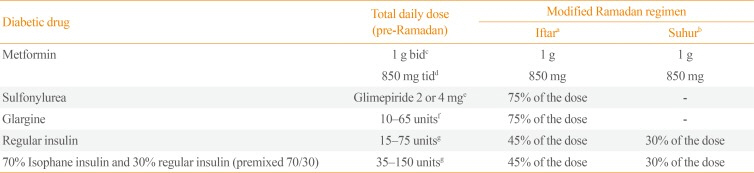
The enrolled patients were then divided into the following four groups according to their medication regimen: group A (metformin, sulfonylurea [glimepiride] and insulin); group B (metformin and sulfonylurea [glimepiride]); group C (metformin and insulin); and group D (insulin alone). Notably, the patients were not started on these drug regimens for the purpose of the study; rather, the groups were devised after enrollment of patients, utilizing only the medications they were already using to ensure the patients' convenience, no one was asked to change the type of drug(s) that he or she was taking; instead, only the dosages were changed. The changes made are summarized in Table 1. Other than these dose modifications, the patients' baseline treatment regimens were kept constant.
The above modifications were decided by the authors of this study and were guided by an unpublished pilot study conducted by the authors during Ramadan 2013, in which two groups of Muslim patients with T2DM and aged 40 to 70 years were prospectively studied. The same inclusion and exclusion criteria as used in the present study were used then, as well as the same anti-diabetic drugs, albeit using different dosing regimens. The first group (n=79) was divided to four subgroups according to their medication regimen, subgroup A (n=19) metformin, glimepiride, and insulin; subgroup B (n=21) metformin and glimepiride; subgroup C (n=20) metformin and insulin; and subgroup D (n=19) insulin alone. The doses of their anti-diabetic drugs were decreased by 50% during Ramadan. The other group (n=75) was also divided to four subgroups: subgroup A (n=18); subgroup B (n=19); subgroup C (n=19); and subgroup D (n=19). The medication regimen of these subgroups was similar to that of the first group. However the doses were decreased by 25% rather than 50%. Although there was no significant difference in the incidence of hypoglycemia, DKA, or NKHS between the two groups, 11 patients from group 1 (five from subgroup C and six from subgroup D) visited the emergency department due to profound hyperglycemia (defined as plasma glucose >400 mg/dL), compared with only one patient from group 2 (subgroup D) (P=0.005).
Study endpoints
The study's primary endpoint was the incidence of hypoglycemia, DKA, or NKHS among the patients during Ramadan compared within the preceding month, serving as measures of the proposed protocol's safety.
Hypoglycemia was defined as a serum glucose level of less than 70 mg/dL [15] along with symptoms or with blood glucose of 60 mg/dL or less regardless of symptoms [16]. Severe hypoglycemia was defined as a hypoglycemic episode requiring assistance from another person [15].
The patients were provided with diary cards to record any symptoms and their timing and were instructed to perform finger-stick glucose measurements (FSGMs) before each meal and at bedtime during the month preceding Ramadan. During Ramadan, the FSGMs were to be obtained before Suhur, at noon, before Iftar and 2 hours post-Iftar. Furthermore, the patients were asked to record the number, details and symptoms of any episodes of hypoglycemia, DKA, and NKHS, in addition to the details of and reasons for any hospital or emergency room visits. Moreover, the patients were scheduled for weekly follow-up visits during Ramadan and the preceding month, at which they were asked about the above information to confirm the data in the diary cards.
At the final follow-up visit at the end of Ramadan, the following information was obtained by means of a questionnaire and an oral interview with one of the authors of this study: confirmation of fasting during Ramadan, the number and details of hypoglycemic episodes, and the development of DKA or NKHS during Ramadan and the preceding month. The patients were also assessed for compliance with their treatment regimens during the study period by reviewing their diary cards.
Statistical analysis
The primary outcomes were the frequency of hypoglycemia, DKA and NKHS before Ramadan and at the end of the 29-day fasting period. Changes in the frequency of hypoglycemia were tested using a binomial test because the counts of subjects with positive responses were small. A P value of less than 0.05 was the cutoff for significance. Backward stepwise regression revealed that the baseline values of the patients' age, HbA1c, body mass index, duration of diabetes, and the patients' sex did not have any relationship with the frequency of hypoglycemia before Ramadan.
RESULTS
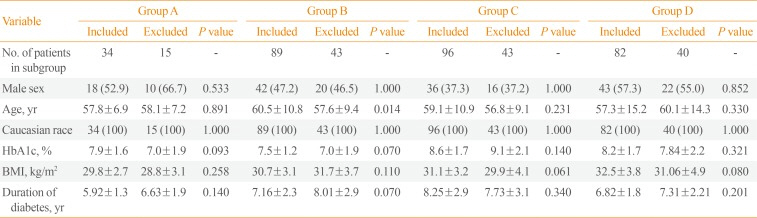
A total of 468 patients were enrolled in the study, of which 167 were excluded from data analysis after enrollment (Fig. 1). Among the excluded patients, 142 were excluded for being lost to follow-up or returning incomplete diary cards, and were distributed equally among the treatment groups (group A, 30.6%; group B, 32.6%; group C, 31.0%; group D, 32.8%; P=0.981), with an overall rate of 31.9%. In addition, there was no statistically significant difference in the baseline characteristics between he included and excluded groups Table 2. The other 25 patients excluded for non-adherence to fasting or non-compliance to medication were not expected to significantly introduce bias. None of the patients died during the study. Of the 301 patients included 139 (46.2%) were male, with a mean age of 58.5±11.2 years. All patients were Arabs.
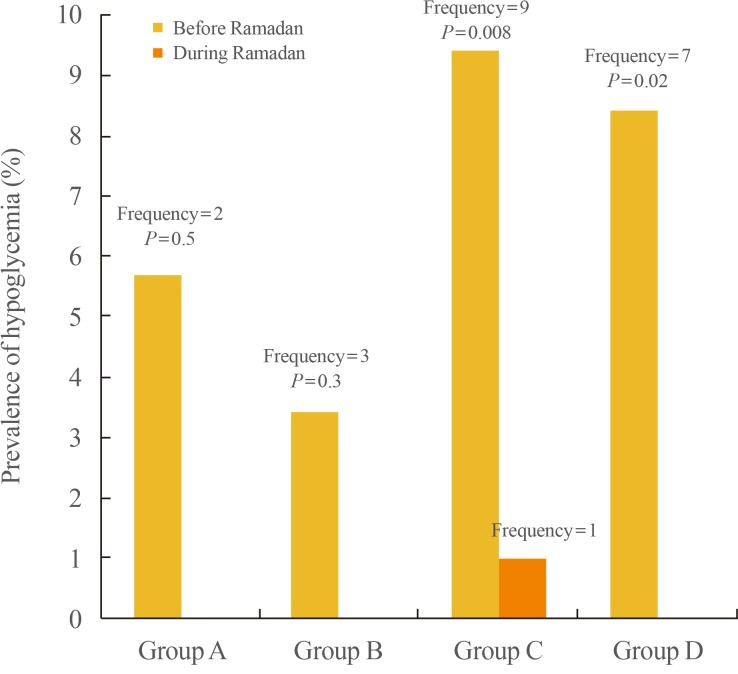
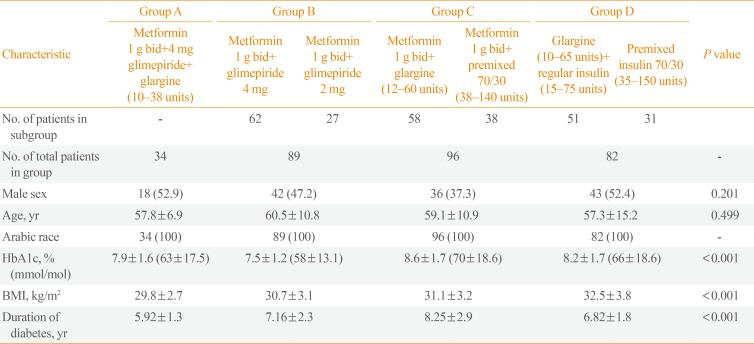
The detailed results for the four categories of patients were as follows (Table 3). Group A received metformin, sulfonylurea, and insulin and included 34 patients. The number of hypoglycemic episodes during the month before Ramadan (pre-Ramadan) was two, compared to none during Ramadan (P=0.498) (Table 4).
Group B (n=89) received metformin and sulfonylurea and was divided into two subgroups according to glimepiride dosage: 62 patients received 4 mg of glimepiride; the rest received 2 mg. Three episodes of hypoglycemia were reported pre-Ra-madan and none during Ramadan (P=0.252).
Group C (n=96) received metformin and insulin. Fifty-eight received insulin glargine, while 38 received premixed insulin 70/30. Nine episodes of hypoglycemia occurred pre-Ramadan and only one episode during Ramadan (P=0.008).
Group D (n=82) received insulin only; 51 patients received insulin glargine plus regular insulin, the rest received premixed insulin 70/30 only. There were seven reported episodes of hypoglycemia pre-Ramadan and none during Ramadan (P=0.016).
No episodes of severe hypoglycemia were observed (Fig. 2); all fell under the category of symptomatic hypoglycemia and were self-treated by the patients without seeking professional medical assistance and with no further complications. The characteristics of the patients who suffered a hypoglycemic episode in each group before and during Ramadan are shown in Table 4. Furthermore, no cases of DKA or NKHS were reported during the study period in any of the treatment groups. A statistical analysis of the demographic data revealed no sources of confounding bias.
DISCUSSION
This prospective, observational, open-label study demonstrated that none of the four groups showed any significant increase in the incidence of the three examined complications: hypoglycemia, DKA, and NKHS. Furthermore, groups C and D showed significant decreases in the incidence of hypoglycemia during Ramadan compared within the preceding month. Therefore, the four proposed drug regimens appear to be safe for use during Ramadan by T2DM patients who choose to fast.
The literature concerning the safety of multi-drug regimens during Ramadan is sparse, with most studies and recommendations focusing on and comparing the safety of monotherapies, rather than multi-drug regimens, during Ramadan [45689111417181920]. Accordingly, many studies have been performed to assess the safety of different anti-diabetic medications during fasting among diabetic patients who insist on fasting during Ramadan [121721]. Many of those studies have reported the incidence of acute glycemic complications (mainly hypoglycemia). Several of those studies were undertaken to compare the safety of one oral anti-diabetic drug with that of another [121721]. Other studies have addressed safety during fasting by switching the dose of an anti-diabetic drug usually taken in the morning to the evening [20]. Other studies have compared hypoglycemic events in patients receiving Humalog Mix 50 (Lilly, Indianapolis, IN, USA) with those in patients treated with human insulin Mix 30 [11].
Metformin is recommended because of the low risk of hypoglycemia associated with its use, although the dose schedule must be altered to accommodate changes in meal patterns during Ramadan [48]. Additionally, many patients with diabetes require additional anti-hyperglycemic medications to manage their disease [22]. Therefore, sulfonylureas are typically recommended in combination with metformin based on broad clinical experience and their low cost [23]. Nevertheless, Salti and Diabetes and Ramadan Study Group [10] reported a hypoglycemia incidence rate of 24% in patients on insulin and sulfonylurea combination therapy during Ramadan. For sulfonylurea and metformin multi-therapy, that figure ranged between 7% and 62% [1213212425262728]; however, the two largest studies reported figures of 13% and 9%, respectively [1328], and these number might reflect the true values more accurately. For insulin mono-therapy, the reported rates of the incidence of hypoglycemia range from 1.6% [11] to 45% [19]. In one study by Cesur et al. [14], 49 T2DM patients who were fasting were treated with glimepiride, repaglinide, or insulin glargine and were compared with 16 non-fasting controls, and no significant difference in the incidence of hypoglycemia between the two groups was found. To the best of our knowledge, no studies concerning the safety of combination therapy with insulin, sulfonylurea, and metformin have been conducted.
A notable discrepancy between the rates of hypoglycemia during Ramadan reported in the current study and those in the literature is thus apparent. It is the opinion of the authors that this difference stems from the proposed modifications to the four drug regimens, especially given that a number of the articles referenced above did not change the dosages of the anti-diabetic drugs for the sampled population, i.e., the patients were kept on their pre-Ramadan regimens in terms of the total doses used [101112212527]. Moreover, the strict exclusion criteria employed in the present study might have played a role in the discrepancy. It could also be argued; however, that a closer patient-physician interaction and the attendance of pre-Ramadan educational sessions by the patients might have confounded the results of this investigation. The positive effects that patient education might have on the rates of hypoglycemia during Ramadan have been reported in literature before [29].
We feel obliged to elaborate on several of this study's strengths and limitations. To the best of our knowledge, there has not been a previous study comparing four different concurrent anti-diabetic regimens including sulfonylurea, metformin, insulin glargine, regular insulin, and/or premixed insulin. Additionally, we sought a practical approach to drug regimen modification, in that only the doses were modified, rather than the drugs themselves, relieving patients of having to learn about new medications. Moreover, in contrast to more expensive anti-diabetic drugs such as rapid acting insulin analogues and incretin based therapies, the drugs included in this study might appeal to a greater audience all the over the world due to less cost and thus easier accessibility.
As for the limitations, first, the study was not designed in a randomized control trial setting, which is the most appropriate for studies comparing different drug regimens. However, due to the limited patient population from which the sample was derived, a control group of similar demographics to the treatment group could not be assembled. The authors thus decided to use the treatment group's pre-Ramadan status as a form of control. Second, we relied on interviews and diary cards for data collection. However, diary cards have been criticized in the past as a method of data collection in terms of the accuracy of the data reported [30]. Of particular concern is the Hawthorn effect, in which individuals modify their behavior in reaction to being observed [31]. However, this false reporting bias in our case was similarly applicable to both months being studied (Ramadan and the preceding month). The authors also missed the opportunity to download data off of the patients' glucometers, which might have provided more evidence based conclusions. We were unable to obtain that data because of the financial limitations of some of the subjects who did not own a glucometer at home. Those patients relied on their neighborhood pharmacies or health centers to check their glucose levels. Third, females of reproductive age were excluded due to their generally shorter fasting period during Ramadan, since they are exempted from fasting during menstrual periods. As a result, the females who were included were all post-menopausal, which skewed the mean age of the sample population and possibly led to a false elevation in the incidence of hypoglycemia because advanced age is itself a risk factor for hypoglycemia. Nevertheless, the average age of the entire sample studied was approximately 59 years, which would classify the sample as middle-aged on average. Fourth, optimal glycemic control could not be accurately evaluated with the use of serum HbA1c since those values reflect the glycemic status of the preceding 3 months. The more suitable test for short term evaluation—serum fructosamine level—was unfortunately unavailable in the country. Finally, the sample sizes of groups A and B were relatively small, and the statistical power was less than 80%. Hence, the small sample size may contribute to the low incidence of hypoglycemia and no report of DKA or NKHS. Of note, analysis of the baseline characteristics of included and excluded patients did not show attrition bias.
In summary, this is the first study that investigated the safety of dose adjustments for four anti-diabetic drug regimens including a total of five drugs in T2DM patients fasting Ramadan. The lack of an increase in the incidence of the hypoglycemia, NKHS, and DKA endorses the safety of the proposed regimens for those patients.
We recommend further research into this subject. Larger studies could be designed with larger sample populations from different geographical locations, comparing the safety of more anti-diabetic drugs. Additionally, the efficacy of the proposed protocol in achieving glycemic control could be further investigated. Finally, studying the group of patients who dropped out and comparing them with the group that remained might be of interest.


 XML Download
XML Download