

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Autoimmune thyroid diseases (AITD) like Graves disease and Hashimoto disease are complex diseases in which autoimmunity against thyroid autoantigens develop against a certain genetic background, provoked by exposure to environmental factors. Weetman [1] has used Swiss cheese as a model to explain the immunopathogenesis of AITD. Swiss cheese has characteristic big holes. Assuming each hole represents a genetic, environmental, or existential factor, the disease may manifest itself when a number of subsequent holes are aligned in a way that an arrow may pass them all in one shot. Table 1 lists these various factors. Thus the autoimmune reaction is facilitated by polymorphisms in major histocompatibility genes (human leukocyte antigen [HLA]), immunoregulatory genes, and thyroid specific genes, probably provoked by various environmental factors and enhanced by existential factors like female gender, parity, and age. Twin studies have indicated that the relative contribution of genetic factors to the development of Graves' hyperthyroidism is about 79% [2]. Likewise, genetic factors would contribute for about 73% to the development of thyroid peroxidase (TPO) antibodies and/or Tg antibodies [34]. The implication is that the proportion of environmental factors in the immmunopathogenesis of AITD is limited, in the order of 20% to 30%. The number of known susceptibility loci increases every year, but taken together accounts for less than 20% of the heritability of AITD [15]. Presumably many more unidentified susceptibility loci are involved.
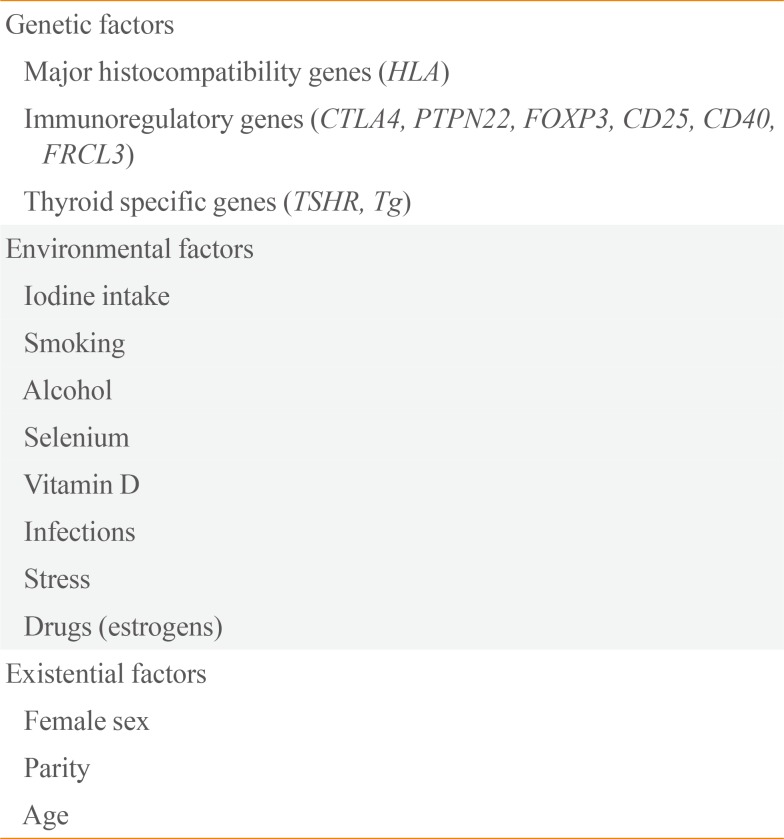
Table 1
Genetic, Environmental, and Existential Factors in the Immunopathogeneis of Autoimmune Thyroid Disease
![]()
AITD frequently runs in families, and having a family member with AITD increases the risk you yourself will get AITD. The risk for siblings of AITD patients can be quantified by the sibling risk ratio λs, defined as the risk for developing AITD in a sibling of an AITD patient divided by the frequency of AITD in the general population. Λs is 16.9 for AITD, 11.6 for Graves' hyperthyroidism, and 28.0 for Hashimoto's hypothyroidism [6]. The λs is a rather rough risk estimate for individual subjects. I have been frequently asked by patients in whom I had just diagnosed overt Graves or Hashimoto disease: "Doctor, I know my thyroid disease runs frequently in families and occurs especially in women. I am concerned about my daughter who is now in her twenties, and planning to become pregnant some years from now. How high is the chance she will also get thyroid disease, and can anything be done to prevent that happening?" Prevention in this context would mean modulation of exposure to particular environmental factors, as changing the genetic make-up of an individual albeit theoretically possible is not that easy. Preventive interventions are likely to be more effective in persons who already carry a somewhat higher risk. Consequently in this review article we will first evaluate the predictability of developing AITD, and thereafter review the role of various environmental factors in the development of AITD. Lastly, a synopsis will be provided what an individual at risk to develop AITD, can do to diminish that risk.
Go to : 
PREDICTION OF AUTOIMMUNE THYROID DISEASE
The Amsterdam AITD cohort is a 5-year follow-up study in a population at risk for AITD, namely in healthy women with one or more 1st or 2nd degree relatives with proven AITD [7]. The study aim was to design a predictive score for the development of overt autoimmune hypo- or hyperthyroidism, and to learn more about the pathogenesis of AITD especially on the role of environmental factors in the early stages of the disease. At study entrance women should be without known thyroid disease and without overt hyper- or hypothyroidism. There were 790 participants with a mean age of 36±12 years and median thyroid-stimulating hormone (TSH) was 1.7 mU/L. Subclinical hyperthyroidism was detected in 13 and subclinical hypothyroidism in 19 participants at baseline. TPO-Ab ≥100 kU/L were present in 27%, Tg-Ab ≥100 kU/L in 8%, a family history of Graves disease in 76% and of Hashimoto disease in 49%. Participants were seen annually for blood sampling and filling in questionnaires. After 5-year follow-up, there had been 38 events of overt hypothyroidism (34×Hashimoto's thyroiditis, 4×postpartum thyroiditis) and 13 events of overt hyperthyroidism (11×Graves' hyperthyroidism, 1×postpartum thyroiditis, and 1×silent thyroiditis). The mean annual event rate was 1.5%, and the 5-year cumulative event rate was 7.5%. The incidence rate per 1,000 women years in the Amsterdam AITD cohort was 9.6 for overt hypothyroidism and 3.3 for overt hyperthyroidism; these figures are about three times higher than observed in population-based studies in the United Kingdom (UK): 3.5 and 4.98 for overt hypothyroidism and 0.8 and 0.77 for overt hyperthyroidism in the Whickham and Tayside regions of the UK, respectively [89].
Independent risk factors for the occurrence of overt hyper- or hypothyroidism in the Amsterdam AITD cohort were baseline TSH, baseline TPO-Ab, and family background of AITD. A predictive score for such events was obtained from a logistic regression model by putting weights to individual risk factors proportional to their relative risk. This so-called Thyroid Events Amsterdam (THEA) score is listed in Table 2. Low scores are associated with a low incidence of overt hyper- or hypothyroidism in the next 5 years, and vice versa [7].
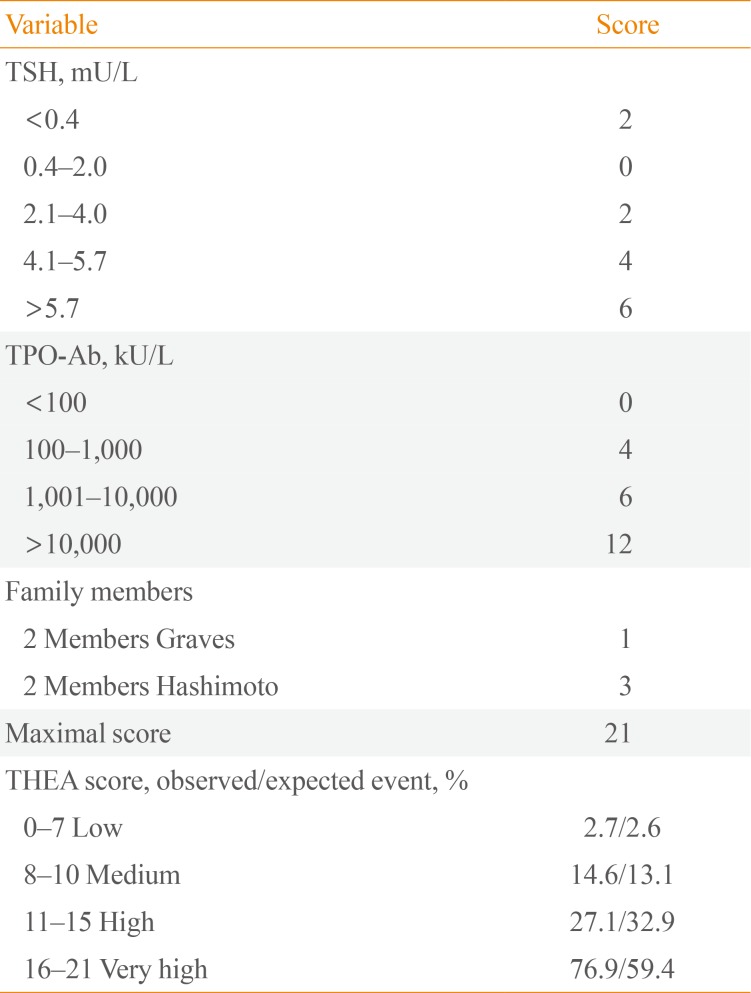
Table 2
The Predictive THEA Score to Estimate the Risk on Developing Overt Autoimmune Hyperthyroidism or Hypothyroidism in the Next 5 Years
Adapted from Strieder et al. [7].
THEA, Thyroid Events Amsterdam; TSH, thyroid-stimulating hormone; TPO-Ab, thyroid peroxidase antibody.
![]()
Getting back to the patient who was concerned about her 23-year old daughter who wanted to become pregnant in the near future, her mother had Graves' hyperthyroidism and her grandmother Hashimoto's hypothyroidism. Thus the daughter scores zero for "family members." Blood sampling was done in the daughter, revealing TSH 2.5 mU/L and TPO-Ab 500 kU/L; the resulting THEA score is 6, meaning a low chance of about 2.7% for developing overt thyroid dysfunction in the next 5 years. Would her TSH have been 6.0 mU/L and her TPO-Ab 1,100 kU/L, then her THEA score of 12 would indicate a much higher risk of about 30%. The next question obviously is whether she can do anything by herself in order to decrease that risk.
Go to :
ENVIRONMENTAL FACTORS IN THE PATHOGENESIS OF AUTOIMMUNE THYROID DISEASE
Iodine intake
It is well known that at a population level thyroid antibodies and autoimmune hypothyroidism are more common in iodine-replete areas than in iodine-deficient areas. The most recent evidence supporting this statement comes from Denmark. The prevalence of TPO-Ab before and after mandatory iodization of salt was 14.3% and 23.8%, respectively [10], and the incidence of overt hypothyroidism increased from 38.3/100.000 per year at baseline to 47.2/100.000 per year 5 to 7 years after iodine fortification of salt [11]. Voluntary iodine prophylaxis in a small Italian community also increased prevalence of TPO-Ab (12.6% vs. 19.5%) and hypothyroidism (2.8% vs. 5.0%) 15 years later [12]. At an individual level, one should follow the World Health Organization recommendation of a daily iodine intake of about 150 µg.
Smoking
It has been known for a long time that smoking is a risk factor for Graves disease [13]. Current smoking increases the risk of Graves' hyperthyroidism about two-fold and of Graves' orbitopathy about three-fold. The effect is dose-dependent, more pronounced in women than in men, and disappears a few years after cessation of smoking. Less well known is the more recent finding that smoking to a certain extent protects against hypothyroidism. Current smokers have a lower prevalence of TPO-Ab as compared to non-smokers, both in the Amsterdam AITD cohort at baseline (odds ratio [OR], 0.69; 95% confidence interval [CI], 0.48 to 0.99) and in the third National Health and Nutrition Examination Survey (OR, 0.57; 95% CI, 0.48 to 0.67) [1415]. In the population-based HUNT study in Norway current smokers as compared to never smokers have also a lower prevalence of subclinical hypothyroidism (OR, 0.54; 95% CI, 0.45 to 0.66) and of overt hypothyroidism (OR, 0.60; 95% CI, 0.38 to 0.95) [16]. The effect is dose-dependent, and disappears a few years after cessation of smoking. In the longitudinal Amsterdam AITD cohort de novo occurrence of TPO-Ab and/or Tg-Ab occurred in 20% of the initially antibody-negative participants during the 5-year follow-up [17].
Participants who stopped smoking in this period increased their risk to develop de novo TPO-Ab and/or Tg-Ab. In the prospective DanThyr study, 140 patients diagnosed with autoimmune hypothyroidism had more often quitted smoking in the last 2 years before diagnosis than 560 matched controls (16.4% vs. 3.4%) [18]. The increased risk of autoimmune hypothyroidism upon quitting was transient: OR's <1 year after stopping smoking, 1 to 2 years after cessation of smoking and 3 to 10 years after quitting were 7.36 (95% CI, 2.27 to 23.90), 6.34 (95% CI, 2.59 to 15.3), and 0.75 (95% CI, 0.30 to 1.87), respectively.
Alcohol
A nested case-control study in the Amsterdam AITD cohort did not find a relationship between alcohol consumption and de novo development of TPO-Ab, but participants who developed overt autoimmune hypothyroidism consumed less alcohol than those who remained euthyroid [19]. A population-based case-control study in Denmark likewise observed that moderate alcohol consumption reduces the risk of overt autoimmune hypothyroidism: OR's were 1.98 (95% CI, 1.21 to 3.33) for 0 alcoholic units/week, 1.00 for 1 to 10 units/week (reference), 0.41 (95% CI, 0.20 to 0.83) for 11 to 20 units/week, and 0.90 (95% CI, 0.41 to 2.00) for ≥21 units/week [20]. Most remarkable, the same group of Danish investigators showed that moderate alcohol consumption also reduces the risk of Graves' hyperthyroidism: OR's were 1.73 (95% CI, 1.17 to 2.56) for 0 units/week, 1.00 for 1 to 2 units/week (reference), 0.56 (95% CI, 0.39 to 0.79) for 3 to 10 units/week, 0.37 (95% CI, 0.21 to 0.65) for 11 to 20 units/week, and 0.22 (95% CI, 0.08 to 0.60) for ≥21 units/week [21]. The observed associations were independent of the type of alcohol (wine or beer did not matter), gender, iodine intake, or smoking behaviour. As there exists a clear association between smoking and alcohol intake, smoking could have been an important confounder in these studies, but that was not observed. The observed association between alcohol intake and AITD likely indicates a cause-and-effect relationship in view of the strength and consistency of the associations and the presence of a dose-response effect. A protective effect of alcohol has also been recorded for other autoimmune diseases like rheumatoid arthritis and type 1 diabetes. The mechanism of action of these protective effects of alcohol remain poorly understood.
Selenium
Glutathione peroxidases and thioredoxin reductases are selenoproteins involved in regulation of the redox state and protection from oxidative damage. The thyroid gland contains more selenium per gram tissue than any other organ. The enzyme GP×3 protects thyrocytes from oxidative stress generated by the action of H2O2. Low selenium levels have been associated with poor immune function. Thus it has been hypothesized that mild nutritional selenium deficiency may promote thyroid autoimmunity. Conversely, selenium supplementation might have a beneficial effect on thyroid autoimmunity, and that has been tested in up to now eight randomized placebo-controlled clinical trials (Table 3). Recruited were patients with Hashimoto's thyroiditis and TPO antibodies. Baseline TSH was either normal or slightly elevated, and exogenous levothyroxine was used by participants in some of the trials. Primary outcome was change in TPO-Ab, which makes sense. For, in the natural history of AITD, TPO-Ab are detectable in serum for a long time (actually for years) with a gradual increase in concentration before serum TSH becomes slightly abnormal (stage of subclinical thyroid dysfunction) and finally serum free thyroxine and/or triiodothyronine become abnormal (stage of overt hypo- or hyperthyroidism) [22]. If selenium could lower the serum concentration of TPO-Ab, one could expect it would slow down the development of thyroid autoimmunity and delay or prevent progress to the stage of subclinical hypo/hyperthyroidism. Unfortunately, the outcome of the trials has not been unequivocal: TPO-Ab concentration decreased in four trials but did not change in another four trials (Table 3) [2324252627282930]. The different outcomes cannot be explained from the applied selenium preparation (sodium selenite or selenomethionine), the concomitant use of L-T4, sample size (although limited in all trials, group sizes were in the same order of magnitude in all studies), baseline selenium concentration and baseline TPO-Ab concentration. Patients with different GP×1 genotypes presented comparable responses in TPO-Ab levels [30]. At present, it cannot be excluded that selenium supplementation will decrease TPO-Ab specifically in regions with iodine deficiency (which increases the amount of oxidative stress to the thyroid gland), or when given for a longer period than 6 months.
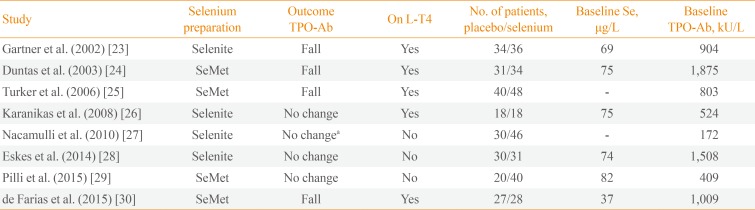
Table 3
Effect of Selenium Supplementation on TPO antibodies in Eight Randomized Clinical Trials
| Study | Selenium preparation | Outcome TPO-Ab | On L-T4 | No. of patients, placebo/selenium | Baseline Se, µg/L | Baseline TPO-Ab, kU/L |
|---|---|---|---|---|---|---|
| Gartner et al. (2002) [23] | Selenite | Fall | Yes | 34/36 | 69 | 904 |
| Duntas et al. (2003) [24] | SeMet | Fall | Yes | 31/34 | 75 | 1,875 |
| Turker et al. (2006) [25] | SeMet | Fall | Yes | 40/48 | - | 803 |
| Karanikas et al. (2008) [26] | Selenite | No change | Yes | 18/18 | 75 | 524 |
| Nacamulli et al. (2010) [27] | Selenite | No changea | No | 30/46 | - | 172 |
| Eskes et al. (2014) [28] | Selenite | No change | No | 30/31 | 74 | 1,508 |
| Pilli et al. (2015) [29] | SeMet | No change | No | 20/40 | 82 | 409 |
| de Farias et al. (2015) [30] | SeMet | Fall | Yes | 27/28 | 37 | 1,009 |
![]()
Selenium supplementation has been beneficial in two other thyroid conditions: it ameliorated and prevented progression of mild Graves' ophthalmopathy [31], and when given to pregnant women it lowered the postpartum surge of TPO-Ab and reduced the incidence of postpartum thyroid dysfunction [32]. It should be realized that these studies have been performed in areas with marginally low selenium blood levels; it is not known if the same favourable results will be observed in selenium- replete areas. Selenium supplementation of 60 µg/day as of 12 to 14 weeks of gestation did not change (as compared to women randomized to receive placebo) the prevalence of TPO-Ab, Tg-Ab, subclinical hypothyroidism, or isolated maternal hypothyroxinemia in the 2nd and 3rd trimester [33].
Most trials on selenium supplementation provided 200 µg/day for 6 months. In the Dutch trial [28], this dose increased plasma Se concentrations from 73 µg/L at baseline to 96 µg/L at 3 months and 95 µg/L at 6 months; obviously a plateau had been reached within 3 months. For people who already have adequate Se intake with their food (especially with baseline Se ≥122 µg/L), selenium supplementation may carry a risk of developing type 2 diabetes [34]. Serum Se concentrations associated with minimal mortality are between 130 to 150 µg/L. There may be health benefits and no extra risk for people with baseline Se <122 µg/L by raising their selenium status, perhaps to 130 to 150 µg/L [34].
Perhaps the strongest circumstantial evidence that selenium intake is associated with thyroid autoimmunity, is derived from a recent population-based study in China [35]. The prevalence of thyroid diseases was compared in two counties, one with an adequate Se intake and the other with a low Se intake. The prevalence of thyroid diseases (except hyperthyroidism, Graves disease, and nodules) was significantly higher in the low Se county (Table 4). Dividing all participants according to their serum Se concentration, those with serum Se in quintile 1 (<47 µg/L) and quintile 2 (47 to 69 µg/L) had higher prevalences of autoimmune thyroiditis, subclinical hypothyroidism, hypothyroidism and enlarged thyroid gland than those in quintile 3 (69 to 90 µg/L), quintile 4 (91 to 119 µg/L), and quintile 5 (≥120 µg/L); prevalences in quintiles 3, 4, and 5 were similar. To prove a causal relationship between low Se intake and thyroid autoimmunity will require preventive intervention randomized clinical trials (RCTs) in this area.
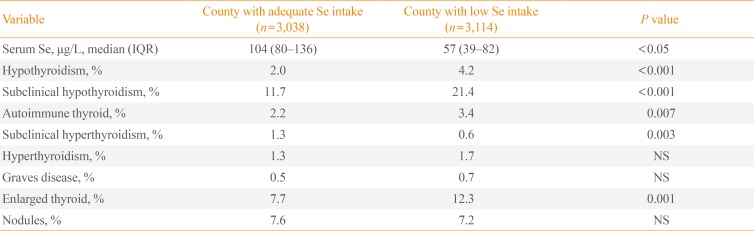
Table 4
Low Selenium Intake Is Associated with High Prevalence of Hashimoto Thyroiditis: A Population-Based Study in China
![]()
Vitamin D
Macrophages, dendritic cells, monocytes, T- and B-lymphocytes express the vitamin D-activating enzyme CYP27B1 and the vitamin D receptor (VDR). The active hormone 1,25(OH)2D (derived either from the systemic circulation of from local conversion of 25(OH)D) binds to VDR, thereby modulating innate and adaptive immune systems [36]. Low vitamin D levels have been identified as risk factors for various autoimmune diseases (like type 1 diabetes, rheumatoid arthritis, and multiple sclerosis). There have been many cross-sectional studies evaluating an association between vitamin D blood levels and AITD, with conflicting results. A meta-analysis of 20 case-control studies revealed lower 25(OH)D levels in AITD patients than controls (standardized mean difference, -0.99 ng/mL; 95% CI, -1.31 to -0.66) [37]. AITD patients (with Graves disease or Hashimoto thyroiditis) were also more likely to have vitamin D deficiency (OR, 2.99; 95% CI, 1.88 to 4.74). A drawback of this meta-analysis is that it did not pay any attention on the many known determinants of serum vitamin D levels, such as age, sex, body mass index (BMI), smoking, estrogen use, and month of blood sampling (in view of substantial seasonal variation). Similar results, however, were observed in a large study among 6,685 Korean subjects undergoing routine health check-ups, which tried to avoid the many confounding factors [38]. Serum 25(OH)D levels were lower in women with TPO-Ab than in women without TPO-Ab (22.0 ng/mL vs. 23.5 ng/mL, P=0.03); the difference was observed in premenopausal women but not in postmenopausal women and men. The prevalence of TPO-Ab in women with vitamin D deficiency (<10 ng/mL), vitamin D insufficiency (10 to 30 ng/mL), and vitamin D sufficiency (>30 ng/mL) was 21.2%, 15.5%, and 12.6%, respectively (P=0.027). OR's adjusted for age, BMI, serum calcium, smoking, menopause, and season were 1.95 for vitamin D deficiency and 1.31 for vitamin D insufficiency (relative to an OR of 1.0 for vitamin D sufficiency).
The only prospective study in this area, however, did not confirm these data. A nested case-control study was performed within the Amsterdam AITD cohort, in which controls were matched to cases (defined as those subjects in whom TPO-Ab developed de novo during follow-up) for age, BMI, smoking, estrogen use, season, and duration of follow-up [39]. Serum 25(OH)D and serum 1,25(OH)2D concentrations were not different between cases and controls, neither at baseline nor at the time of the occurrence of TPO-Ab. The issue may become even more complicated by the finding that particular polymorphisms in the VDR gene are associated with AITD [40]. So far, there has been no studies to evaluate the effect of vitamin D supplementation on thyroid autoimmunity.
Infections
Infections have been implicated in the pathogenesis of AITD [41]. The best studied infection in this regard is that with Yersinia enterocolitica. There is a sound biologic rationale for a causal link between Y. enterocolitica infection and AITD. Y. enterocolitica has specific binding sites for TSH, which are recognized by TSH receptor antibodies isolated from patients with Graves disease. Conversely, immunization of mice with Y. enterocolitica leads to the induction of TSH receptor antibodies. YOP (Y. enterocolitica outer membrane protein) antibodies stain thyroid epithelial cells in immunochemistry. The Y. enterocolitica protein cross-reacting with TSH receptors has recently been identified: the YOP membrane porin F shared cross-immunogenicity with a leucine-rich domain of the TSH receptor [42]. The plausible theory then is that Y. enterocolitica ompF (outer membrane porin F) is involved in the production of TSH receptor antibodies and the pathogenesis of Graves disease through molecular mimicry. However, recent epidemiological studies do not support this theory. A nested case-control study in the Amsterdam AITD cohort looked into de novo occurrence of TPO-Ab in relation to Y. enterocolitica infection [43]. The proportion of subjects with YOP antibodies (IgG and IgA) did not differ between cases (those who developed TPO-Ab) and controls (those who remained TPO-Ab negative), at baseline, at 1 year before seroconversion, and at the time of seroconversion. The same negative results were obtained when analysing hypothyroid and hyperthyroid cases with their respective controls. The data argue strongly against a causative role of Y. enterocolitica infection in the pathogenesis of AITD. In contrast, a recent Danish paper in twin pairs discordant for Graves disease concludes "that Y. enterocolitica infection plays an etiological role in Graves disease or vice versa," based on a higher frequence of chronic Y. enterocolitica infection (reflected by the presence of both IgA and IgG YOP antibodies) in patients with Graves disease than in controls [44]. The Danish findings, however, are in good agreement with a previous cross-sectional study in the Amsterdam AITD cohort at baseline, in which the prevalence of YOP IgG and IgA in AITD relatives was also higher than in controls [45]. The increased prevalence of YOP antibodies (which are not related to higher prevalence of TPO-Ab) suggest a higher rate of persistent Y. enterocolitica infection in AITD relatives. Susceptibility genes for AITD may also confer a risk to Y. enterocolitica infection.
Stress
Stress as a provocative factor in the pathogenesis of Graves disease is well known. A number of case-control studies report a higher frequency of stressful life events in the year preceding the diagnosis of Graves' hyperthyroidism relative to controls [46474849]. These studies were all retrospective in nature, and therefore the obtained evidence is at best circumstantial. Stress exposure in subjects developing Hashimoto's thyroiditis has hardly been studied. The Amsterdam AITD cohort assessed recent life events (both pleasant and unpleasant) and daily hassles by means of annual questionnaires during the 5-year follow-up. Two nested case-control studies in the cohort did not find any association between stress exposure and de novo occurrence of TPO-Ab or the development of overt autoimmune hypothyroidism [50].
Drugs
Interferon-α, alemtuzumab, and highly active anti-retroviral therapy are capable to induce AITD, either Hashimoto or Graves disease. Of more relevance in the current review are estrogens, used by women as contraception in their reproductive phase or as hormone replacement in the postmenopauze. A cross-sectional analysis of the Amsterdam AITD cohort at baseline indicated a lower frequency of estrogen use in euthyroid women with TPO-Ab as compared to TPO-Ab negative women: OR 0.58 (95% CI, 0.35 to 0.97) for ever estrogen use, and 0.81 (95% CI, 0.56 to 1.19) for current estrogen use [14]. The ever use of estrogen seemed also to protect against the development of subclinical or overt hyperthyroidism (OR, 0.17; 95% CI, 0.05 to 0.52) but not against autoimmune hypothyroidism [14]. Prospective nested case-control studies in the Amsterdam AITD cohort observed a borderline association (P=0.06) between current estrogen use and de novo occurrence of TPO-Ab and/or Tg-Ab, but a protective effect of estrogens on development of hyper- or hypothyroidism was not present [17].
Results in the literature have been conflicting as well. A Danish cross-sectional population-based study found no association between oral contraceptive use and thyroid antibodies in women 18 to 45 years old, but postmenopausal women 60 to 65 years who had used or were still using hormone replacement therapy had a lower prevalence of Tg-Ab but not of TPO-Ab [51]. Another study, however, reports no difference in frequency of TPO-Ab and/or Tg-Ab in postmenopausal women with or without hormonal replacement therapy [52]. An early large study reports a lower incidence of hypo- and hyperthyroidism in oral contraceptive users than in controls (relative risk, 0.68; 95% CI, 0.52 to 0.85) [53]. A large population-based Danish study observes a protective effect of the use of oral contraceptives for the development of Graves disease (OR, 0.68; 95% CI, 0.49 to 0.93) but not for Hashimoto disease [54].
Exogenous estrogens thus to a certain extent may protect against the development of thyroid antibodies (more so against Tg-Ab than to TPO-Ab) and against Graves' hyperthyroidism. Oral contraceptives protect against pregnancy, thereby diminishing the risk of AITD. For, the postpartum period carries a risk for the onset of Graves disease [55] and postpartum thyroiditis is often the forerunner of permanent autoimmune hypothyroidism [56].
Go to :
PREVENTIVE INTERVENTIONS IN AUTOIMMUNE THYROID DISEASE
Which preventive interventions can be taken by subjects who are at risk to develop AITD? Table 5 gives an overview of possible interventions that modulate exposure to environmental factors which are likely involved in the immunopathogenesis of AITD [57].
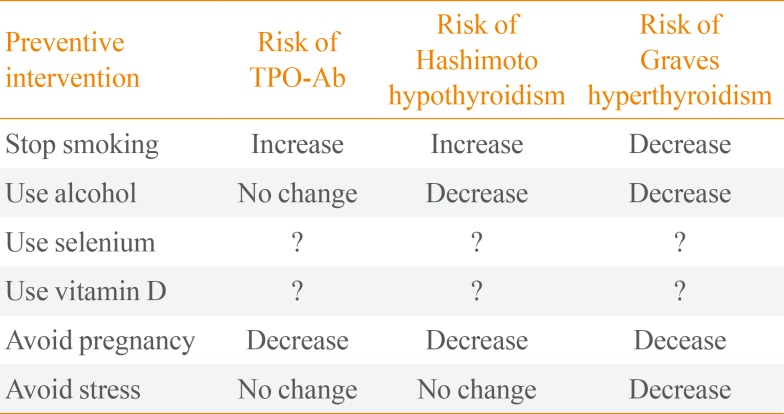
Table 5
Modulation of Exposure to Environmental Factors in Order to Decrease the Risk of Developing Autoimmune Thyroid Disease
![]()
The advice to stop smoking should be given always to every subject. Cessation of smoking will decrease the risk of Graves' hyperthyroidism and even more so of Graves' ophthalmopathy, but the irony is that you lose the protective effect of smoking on Hashimoto's thyroiditis. Moderate use of alcohol seems to protect against both Graves and Hashimoto disease; although, this recommendation will be welcomed by many subjects, drinking alcohol has negative effects as well. Selenium supplementation has been studied extensively in RCTs, but there is still no convincing evidence that increasing selenium intake may prevent a rise of TPO-Ab and thereby the development of subclinical hypothyroidism. Taking 200 µg of selenium daily is unlikely to do harm if baseline serum selenium concentration is lower than 120 µg/L, but carries a risk of type 2 diabetes at higher concentrations. An association between low vitamin D levels and thyroid autoimmunity is likely, but there have been no intervention studies to evaluate whether vitamin D supplementation decreases the risk of thyroid autoimmunity; until such studies have been done, I would not recommend vitamin D for this indication. To avoid pregnancy will indeed decrease the risk of AITD, but that kind of recommendation is not very realistic. And lastly, to avoid stress is likely to diminish the risk of Graves disease, but how do you manage to banish stressful life events and daily hassles from your life?
Taken together, preventive interventions to diminish the risk of AITD are few, not always feasible, and probably of limited efficacy.
Go to :
 XML Download
XML Download