

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Sulfonylureas are the most widely used antidiabetic agents worldwide; however, concern has been raised about their possible adverse effects. These agents may cause weight gain, hypoglycemia, and β-cell exhaustion, resulting in limited effectiveness (secondary failure) long-term [1,2,3]. Therefore, there is interest in hyperglycemic agents with comparable glucose lowering efficacy to sulfonylureas, but with less effect on hypoglycemia and weight gain, which would improve the management of patients with type 2 diabetes mellitus.
Dipeptidyl peptidase-4 (DPP-4) inhibitors have become a commonly used treatment for type 2 diabetes [4], and among these inhibitors, sitagliptin was the first approved agent. It acts by preventing degradation of glucagon-like peptide-1 (GLP-1), thus potentiating the action of native GLP-1 by 2- to 3-fold. Sitagliptin causes glucose-dependent insulin secretion, decreases hepatic glucose output, and may have a trophic effect on pancreatic β-cells [5]. DPP-4 inhibitors are weight-neutral, and the incidences of hypoglycemia and adverse gastrointestinal effects in response to sitagliptin are similar to those with a placebo [6]. In addition, DPP-4 inhibitors increased the number of pancreatic β-cells and improved their function in a preclinical study [7].
While both sulfonylureas and DPP-4 inhibitors increase insulin release from pancreatic β-cells, their underlying mechanisms differ. Thus, it might be possible to replace a sulfonylurea with a DPP-4 inhibitor in certain patients with a high risk of hypoglycemia, but few relevant studies have been conducted. Thus, we investigated the efficacy and safety of sitagliptin when patients switched from a sulfonylurea to sitagliptin and identified good candidates for the drug switch to prevent symptomatic hypoglycemia.
METHODS
Study design
This study was performed in patients with type 2 diabetes mellitus who visited the outpatient Division of the Endocrinology and Metabolism at Severance Hospital, Yonsei University College of Medicine from October 2008 to December 2009. This protocol was approved by the Institutional Review Board of Yonsei University College of Medicine. Patients with symptomatic hypoglycemia, defined as an event with subjective symptoms of hunger, anxiety, sweating, tremors, or palpitations, were switched from glimepiride with metformin to sitagliptin with metformin without a change in the metformin dose. Patients who discontinued sitagliptin before 24 weeks or who changed the dose of their antidiabetic medication during the study period were excluded. The sitagliptin dose was 100 mg once daily. All subjects were tested for serum glycated hemoglobin (HbA1c), fasting plasma glucose (FPG), and 2-hour postprandial plasma glucose (2h-PPG) before and 12 and 24 weeks after the drug switch.
We divided the patients into two groups based on their status of glucose control at 12 or 24 weeks after the drug switch to identify good candidates for the switch (HbA1c ≤7% [adequate control group, group 1] vs. HbA1c >7% [inadequate control group, group 2]). Factors affecting the efficacy of switching to sitagliptin were evaluated. The clinical parameters assessed in the two groups included age, sex, duration of diabetes, body mass index (BMI), plasma lipid concentration, pancreatic β-cell function, and degree of insulin resistance.
The patients' records were reviewed to verify the duration of diabetes and medication profiles. We calculated the BMI of the participants using the height and weight measurements from these records. FPG/2h-PPG levels were determined using a standard glucose oxidase method and a 747 automatic analyzer (Hitachi Instrument Service, Tokyo, Japan). Plasma triglycerides, total cholesterol, and high density lipoprotein cholesterol were assayed using a routine Hitachi 7600 autoanalyzer (Hitachi Instrument Service). Low density lipoprotein cholesterol was calculated using the Friedewald equation. HbA1c level was measured by high-performance liquid chromatography using a Variant II Turbo system (Bio-Rad Laboratories, Hercules, CA, USA). The HbA1c assay was certified by the National Glycohemoglobin Standardization Program [8]. Serum insulin and C-peptide levels were measured in duplicate using an immunoradiometric assay method (Beckman Coulter, Fullerton, CA, USA). Insulin resistance was assessed using the homeostasis model assessment of insulin resistance (HOMA-IR) equation as follows: HOMA-IR=[fasting insulin (µIU/mL)×fasting serum glucose (mmol/L)/22.5]. HOMA-β was calculated to assess pancreatic β-cell function using the following formula: 20×fasting insulin (µIU/mL)/fasting glucose (mmol/L)-3.5 [9,10].
Statistical analysis
Continuous variables with a normal distribution have been expressed as means±SD and discrete variables as percentages. Statistical comparisons of HbA1c, FPG, and PPG levels at 12 weeks and 24 weeks after switch were performed using paired t test. Intergroup differences in baseline characteristics were analyzed by Student t test for continuous variables or the chi-square test for gender. Multivariate logistic regression analysis was used to examine the independent factors for predicting the efficacy when switching from a sulfonylurea to sitagliptin. All statistical analyses were performed using PASW statistics version 18.0 (IBM Co., Armonk, NY, USA). A P<0.05 was considered significant.
RESULTS
Baseline characteristics
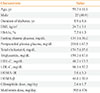
Sixty-one subjects (25 men and 36 women; mean age, 59.3±11.6 years) were switched from glimepiride to sitagliptin due to hypoglycemia and the treatment continued for at least 24 weeks during the study period. Before the switch to sitagliptin, the mean HbA1c value was 7.5%±1.3%, FPG was 134.1±36.0 mg/dL, and 2h-PPG was 218.0±67.5 mg/dL. The mean BMI was 24.7±3.1 kg/m2, and the mean diabetes duration was 8.9±8.6 years. The mean dose of glimepiride before the switch was 2.6±1.7 mg/day, and the mean dose of metformin was 995±476 mg/day (Table 1).
Efficacy and safety after the switch from a sulfonylurea to sitagliptin
The HbA1c level was 7.4%±1.4% at 12 weeks after the switch from glimepiride to sitagliptin and tended to decrease (7.3%±1.2%) after 24 weeks (P=0.8, P=0.241, respectively). FPG was also comparable before and after switching drugs (134.1±36.0 mg/dL at baseline, 137.2±37.8 mg/dL at 12 weeks after switching, 135.0±32.1 mg/dL at 24 weeks after switching). However, the switch from glimepiride to sitagliptin significantly reduced the 2h-PPG level by 21 mg/dL (218.0±67.5 to 197.1±69.9 mg/dL, P=0.045) at week 12 and by 26 mg/dL (218±67 to 192.3±67.4 mg/dL, P=0.018) at week 24 (Fig. 1). The proportion of patients who reached the target HbA1c level of <7% was 31.1% at baseline, which increased to 44.3% and 42.6% at 12 and 24 weeks, respectively. All but one patient stopped experiencing hypoglycemia after discontinuing the sulfonylurea.
Predictive clinical characteristics of sitagliptin after the switch from the sulfonylurea
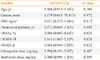
We divided the patients into two groups based on their status of glucose control at 12 weeks after switching drugs to evaluate the clinical factors affecting efficacy after the switch (HbA1c ≤7% [adequate control group, group 1] vs. HbA1c >7% [inadequate control group, group 2]). In both groups, the HbA1c level did not increased with switching drugs. The HbA1c level was 6.8%±0.9% at baseline, 6.4%±0.4% at 12 weeks after switching, and 6.5%±0.5% at 24 weeks after switching in group 1 and 8.0%±1.4% at baseline, 8.2%±1.4% at 12 weeks after switching, and 8.0%±1.2% at 24 weeks after switching in group 2 (Fig. 1). The glycemic profiles and the baseline HbA1c, FPG, and 2h-PPG levels were better in group 1 than in group 2; however, other clinical parameters, including age, duration of diabetes, BMI, HOMA-IR, HOMA-β, and the doses of metformin and glimepiride, did not differ between the two groups (Table 2). A multivariate logistic regression analysis was performed to predict HbA1c levels of ≤7% at 12 weeks after the switch from glimepiride to sitagliptin to identify the best candidates for the switch (Table 3). Age, sex, BMI, duration of diabetes, doses of glimepiride and metformin, baseline HbA1c, HOMA-IR, and HOMA-β were used as independent variables. After adjusting for other factors, a low baseline HbA1c level and high HOMA-IR were predictors of efficacy after switching from glimepiride to sitagliptin.
DISCUSSION
We analyzed 61 Korean patients with type 2 diabetes who switched from glimepiride to sitagliptin because of clinical hypoglycemia. We investigated the efficacy and safety of sitagliptin treatment and identified good candidates for the drug switch. The mean duration of diabetes was approximately 8 years, and these patients were treated with glimepiride and metformin combination therapy. Glycemic control was acceptable, indicated by a mean HbA1c level of approximately 7.5%; however, symptomatic hypoglycemia was evident. The switch did not aggravate glycemic control, and there was a trend towards decreasing HbA1c levels, by 0.1% and 0.2% after 12 and 24 weeks, respectively. The proportion of patients who reached the target HbA1c level of <7% increased from 31.1% to 44.3% after switching drugs. While FPG did not change, 2h-PPG and symptomatic hypoglycemia decreased significantly. These results suggest that patients with dominant insulin resistance, particularly those with frequent hypoglycemia or a high risk for hypoglycemia, may benefit from switching drugs.
Sulfonylureas exert their antihyperglycemic action by stimulating pancreatic β-cells to produce insulin. These agents are a proven and potent therapy for patients with type 2 diabetes mellitus. However, hypoglycemia is a common side effect of these drugs. Hypoglycemia is related to poor clinical outcomes including increased risk for cardiovascular disease and overall mortality in patients with type 2 diabetes [11,12,13]. Furthermore, β-cell preservation is another critical problem, and treating patients with sulfonylureas often results in secondary failure. Secondary failure has two major causes: eventual exhaustion of β-cells caused by the sulfonylurea treatment itself and glucose toxicity induced by poor glycemic control, resulting in reduced pancreatic β-cell responsiveness [14,15]. Sitagliptin, a DPP-4 inhibitor, has recently been used widely to increase insulin secretion in a glucose-dependent manner, potentially presenting a good choice for glucose control with a low risk of hypoglycemia. Several preclinical studies have shown that DPP-4 inhibitors increase the number of pancreatic β-cells and improve their function [7,16,17]. Shirakawa et al. [18] reported the protective effects of DPP-4 inhibitors against increased β-cell apoptosis induced by dietary sucrose and linoleic acid in a mouse model of diabetes mellitus. Several studies have compared the efficacy of DPP-4 inhibitors and sulfonylureas. Arechavaleta et al. [19] showed that adding sitagliptin or glimepiride led to similar improvements in glycemic control in patients with type 2 diabetes on metformin monotherapy. Another study showed that the addition of sitagliptin, compared with glipizide, produced the same results [20]. Sitagliptin was generally well tolerated in both studies, with a lower risk of hypoglycemia and weight loss compared with the two sulfonylureas glimepiride and glipizide. The rate of severe hypoglycemia was as high as 1.5% over 2 years with sulfonylurea use but was very rare with DPP-4 inhibitor use. Considering the results of those studies, DPP-4 inhibitors appear to be possible replacements for sulfonylureas due to their comparable efficacy and obvious superiority in terms of adverse effects and long-term β-cell preservation.
Many efforts have been made to evaluate the efficacy of DPP-4 inhibitors after combining them with another oral hypoglycemic agent, such as metformin, or using them as monotherapy. We evaluated the switch from a sulfonylurea to a DPP-4 inhibitor in an actual clinical setting, particularly in patients with frequent hypoglycemia. Kim et al. [21] showed that switching from a low dose sulfonylurea (average dose of 1.8 mg glimepiride and 30 mg gliclazide modified release) did not change the HbA1c or FPG levels. Chung and Lee [22] reported similar results in 45 patients who switched from glimepiride (average dose, 3.44 mg/day) to sitagliptin. In addition, they suggested considering a switch in relatively well-controlled patients with frequent hypoglycemia [22]. Our results show that the overall glycemic control was not aggravated. Furthermore, postprandial glycemic control improved in patients who switched from glimepiride to sitagliptin. Many studies have reported postprandial hyperglycemia as a major cause of adverse cardiovascular disease in patients with diabetes mellitus [23]. In addition, variations in glucose contribute to the development and progression of atherosclerosis [24]. Thus, strategies to improve postprandial hyperglycemia and reduce variations in glucose are an important focus in diabetes management. In this study, 2h-PPG decreased by >20 mg/dL after the drug switch. We did not check the exact variations in glucose; however, it can be inferred that sitagliptin reduced glucose excursions in these patients according to the slightly increased FPG level and markedly decreased 2h-PPG level. Thus, this may be another benefit for postprandial glucose control after switching to a DPP4-inhibitor.
We also identified good candidates for the switch from a sulfonylurea to sitagliptin. In previous clinical studies, high baseline HbA1c [25,26], low insulinogenic index [26], short duration of diabetes [21,26], and high BMI [27] were predictors of sitagliptin efficacy. However, our study was different in that we did not use add-on therapy at the time of the sulfonylurea-to-sitagliptin switch. In our study, patients with high HOMA-IR, an insulin sensitivity marker, achieved good glycemic control after the switch to sitagliptin. DPP-4 inhibitors are well known to improve β-cell function [28,29]; however, improvements in insulin sensitivity remain controversial [25,30]. Hyperglycemia in patients with type 2 diabetes is caused by multiple defects, including insulin resistance, impaired insulin secretion, and excessive hepatic glucose production. Sulfonylureas are representative oral hypoglycemia agents without insulin sensitizing effects. However, incretin has pleiotropic effects in addition to an insulin secretory effect [31]. A recent rodent animal model study reported that sitagliptin monotherapy improved insulin sensitivity, as assessed by HOMA-IR, and that this improvement was comparable to that using metformin monotherapy [32]. Thus, if a patient has both insulin resistance and a β-cell secretory defect, a sulfonylurea would improve insulin secretion only; however, sitagliptin may influence both defects, resulting in a greater reduction in HbA1c after drug switching. Our results suggest the clinical implications for this effect.
This study had certain limitations. First, only a relatively small number of cases were included. Second, the definition of hypoglycemia was not accurate, and there was little documentation on weight changes in patients before and after switching drugs. Third, we did not use a standardized meal when assessing 2h-PPG levels, nor did we measure HOMA-IR or HOMA-β after switching drugs. Last, we could not compare the effects of drug switching with a control group because of the retrospective nature of the study. Despite these limitations, our results suggest that it is possible for patients with type 2 diabetes mellitus to switch from a low-dose sulfonylurea to a DPP-4 inhibitor, particularly those with a high risk for hypoglycemia while using a sulfonylurea. Of course, there is concern about the cost. Sulfonylureas offer an inexpensive and effective therapy option for a worldwide pandemic. However, the switch to a safer DPP-4 inhibitor could be another choice to treat patients with a higher risk of hypoglycemia, including elderly, lean, or impaired renal function patients. DDP-4 inhibitors and GLP-1 analogs have gained a significant market share in the USA [33].
In conclusion, glycemic control was not aggravated, and 2h-PPG improved 24 weeks after switching from glimepiride and metformin to sitagliptin and metformin. Approximately half of the patients achieved the goal of an HbA1c level ≤7% after the switch. Both documented and clinical hypoglycemia decreased remarkably after the drug switch. Patients with dominant insulin resistance could be good candidates for switching from a sulfonylurea to sitagliptin.


 XML Download
XML Download