

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Despite recent advances, diabetes is a complex condition to treat in clinical practice, and mortality remains high. Diabetic complications may play an important role in increasing mortality of diabetic patients. The mechanisms underlying the role of hyperglycemia in diabetic complications remain incompletely explained, which means potential involvement of genetic factors in diabetic complications. The vitamin D endocrine system is associated with various disease including diabetes, cancer, cardiovascular disorder, metabolic syndrome, autoimmune disorders, and tuber-culosis [1234]. Active vitamin D mediates its biological effects by binding to the vitamin D receptor (VDR), which is located in the nuclei of target cells. VDR is associated with insulin secretion and sensitivity, also it is expressed in the pancreas. These results show that VDR is a possible role in the development of diabetes.
To date, more than 25 different polymorphisms have been mapped to the VDR locus. The human VDR gene is located on chromosome 12q13.1. It has at least 5 promoter regions, 8 protein-coding exons and 6 untranslated exons, which are alternatively spliced into FokI (in exon 2), BsmI and ApaI (both in intron 8), and TaqI (in exon 9). Recently, there are several reports these VDR polymorphisms are associated with type 2 diabetes, insulin secretion [5678910]. Also, VDR polymorphisms are related with metabolic syndrome, metabolic changes related with obesity and diabetic retinopathy. These studies suggested that VDR polymorphism may play a possible role in the development of diabetic complications. Although, there is insufficient studies of association between VDR polymorphism and Korean type 2 diabetes patients.
In this study, we evaluate the association of VDR polymorphism with diabetic complications in Korean type 2 diabetes patients.
METHODS
The study was designed as a case-control study, which enrolled 537 of patients with type 2 diabetes in Chungbuk National University Hospital. The study was approved by the International Review Board of Chungbuk National University Hospital and all patients gave informed consent prior to being included in the study.
Diagnosis of type 2 diabetes was based on the World Health Organization criteria for diabetes. Diabetic retinopathy was assessed through dilated pupils by trained ophthalmologists and classified as no apparent diabetic retinopathy (mild to moderate, severe), non-proliferative diabetic retinopathy, or proliferative diabetic retinopathy, which were based on the International Clinical Retinopathy Severity Scale. Diabetic nephropathy was defined by the presence of microalbuminuria or overt albuminuria and elevated creatinine level. The macrovascular complications including coronary heart disease or stroke were assessed by the medical records. All subjects underwent biochemical tests, medical history and family history of diabetes. Patients were divided into two groups according to presence of B allele (BB or Bb genotype vs. bb genotype). We compared the clinical characteristics and prevalence of diabetic complications according to presence of B allele.
Genotyping
The genomic DNA was isolated from peripheral leukocytes obtained from ethylenediaminetetraacetic acid-treated whole blood. Polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP) was used to determine the Bsm1 VDR gene polymorphism. The primers for VDR gene was designed based on previous literature. The following Bsm1 primers were used for amplification: forward 5'-CAACCAAGACTACAAGTACCGCGTCAGTGA-3´ and reverse 5'-AACCAGCGGAAGAGGTCAAGGG-3'. The PCR was conducted in a 25 µL volume, with an initial denaturation of 3 minutes at 94℃, followed by 30 seconds denaturation at 94℃, 30 seconds annealing at 62℃, and 1 minute extension at 72℃ for 30 cycles, and a final extension of 5 minutes at 72℃. The PCR products were digested overnight at 37℃ by Fermentas restriction enzymes, and resolved in 1.5% agarose gel ethidium bromide by electrophoresis for genotype analysis. Digestion with Bsm1 yields 3 genotypes: BB (825 bp), Bb (825, 650, 175 bp), and bb (650, 175 bp) (Fig. 1).
Statistical analysis
Hardy-Weinberg equilibrium was tested to evaluate the relationship between gene frequencies and genotype frequencies. The data was expressed as mean±standard deviation.
The clinical characteristics of the patients were compared using the chi-square test for categorical variables and Student t test for continuous variables (Table 1). Multivariate analysis was using the logistic regression to adjust interaction effect of metabolic risk factors to diabetic complication outcomes (Table 2). P values of <0.05 were considered statistically significant. All statistical analyses were performed using SPSS version 15.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
Clinical characteristics
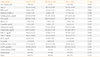
The clinical and biochemical characteristics of the patients are summarized in Table 1. The mean age of the patient population was 62.44±10.64 years, body mass index (BMI) was 25.02±3.64 kg/m2, duration of diabetes was 13.65±7.39 years. There was no difference in sex, duration of diabetes, family history of diabetes and concurrent hypertension, dyslipidemia in between two groups, but results showed significant difference in age (P=0.007), BMI (P=0.002) between two groups (Table 1).
Bsm1 polymorphism and diabetic retinopathy
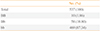
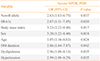
The genotypic distribution of Bsm1 met Hardy-Weinberg equilibrium. The frequency of Bsm1 genotype in patients was as follows: BB, 1.86% (n=10); Bb, 10.80% (n=58); bb, 87.34% (n=469) (Table 3). Patients with BB or Bb genotype was significantly associated with lower risk of diabetic retinopathy compared with patients with bb genotype (BB or Bb genotype 7.4% vs. bb genotype 82.7%, P=0.035) (Table 4).
In logistic regression analysis, B allele was associated with the lower risk of diabetic retinopathy in this study (odds ratio, 2.63; P=0.037). And this association continued after adjusted with other clinical factors (Table 4). Multivariate logistic regression analysis with an enter method was used to evaluate the effect of other clinical factors. In baseline characteristics, there was significant difference with age and BMI between two groups, but after adjustment with these factors, the association with diabetic retinopathy and Bsm1 type still continued (Table 4).
The retinopathy divided to two groups, one is no apparent diabetic retinopathy and mild to moderate non-proliferative retinopathy and the other is severe non-proliferative retinopathy and proliferative retinopathy. Because of some confused description of severities of non-proliferative retinopathy (mild, moderate), but severe retinopathy and proliferative retinopathy may lead to significant consequence (laser treatment or surgery), so this two groups' separation was clinically significant.
Bsm1 polymorphism and diabetic microvascular and macrovascular complications
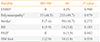
We also evaluate the association of Bsm1 polymorphism and diabetic nephropathy, neuropathy, diabetic foot, coronary artery disease, stroke, and peripheral artery disease. There was no association between the Bsm1 polymorphism and diabetic macrovascular complication, nephropathy, neuropathy, and diabetic foot (Table 2).
DISCUSSION
We evaluated the association of Bsm1 polymorphism with diabetic complications in Korean type 2 diabetic patients. Patients with B allele (BB or Bb) were significantly associated with lower risk of diabetic retinopathy compared with patients without B allele (bb). It showed that B allele in VDR may be a protective factor in the development of diabetic retinopathy. There are a few data about the association with Bsm1 polymorphism and diabetic retinopathy. Bucan et al. [11] showed that bb genotype in VDR has a higher risk of developing diabetic retinopathy. But they didn't show that the association of b allele and diabetic retinopathy. Although Capoluongo et al. [12] did not find Bsm1 association with diabetic complications in the Italian population. Cyganek et al. [5] also reported the same results that no association was observed between the Bsm1 polymorphism and diabetic retinopathy. The relationship of Bsm1 polymorphism with diabetic retinopathy is still controversial. The discrepancies of these results were likely due to the difference in ethnicity or enrolled characteristics of subject among studies.
Diabetic microvascular complications result from several mechanisms including hyperglycemia, hypertension, seem to be also affected by genetic factors. There are several genes about the development of diabetic microvascular complications including endothelial physiology, vasoconstriction, coagulation, oxidative processes, and growth factors. Vitamin D is well known for maintaining normal homeostasis of calcium and phosphorus also has anti-proliferative, anti-angiogenic effect and apoptosis process. The active form of this vitamin D through a specific VDR, VDR is widely expressed in human tissues and organs, including retina. As mentioned earlier, vitamin D has anti-proliferative action in vitro; vitamin D inhibits vascular smooth muscle cell growth and effects on endothelial physiology. Therefore, it is postulated that VDR polymorphism may influence on the development of diabetic retinopathy.
In this study, we demonstrated of possible association with B allele and lower risk of diabetic retinopathy. And this result was about Korean population, there was no previous study about association with diabetic complication and VDR polymorphisms.
We try to evaluate another association in diabetic complication, such as nephropathy, macrovascular complications. There was no association between Bsm1 polymorphism and diabetic nephropathy (end-stage renal disease, P=0.580; normo-/micro-/macroalbuminuria, P=0.302). Zhang et al. [8] reported that B allele in Bsm1 is correlated with large amount albuminuria in the Han Chinese population with type 2 diabetes, and is probably a risk factor for early-onset diabetic nephropathy. Contrary to our result, this study showed that B allele could be responsible for the pathogenesis of early-onset diabetic nephropathy. Bucan et al. [11] showed that no association was observed between Bsm1 genotype and diabetic nephropathy, in common with our data. Marco et al. [13] reported that the greater prevalence of ischemic heart disease and death from cardiovascular causes in BB and Bb genotypes. They suggested that the Bsm1 VDR polymorphism might affect cardiovascular morbidity or mortality through calcium metabolism or VDR mediated influence of 1, 25-dihydroxyvitmain D3 on vascular smooth muscle cells and myocytes. Gyorffy et al. [14] showed that patient with the BB genotype in VDR have a higher risk of development in coronary artery disease. In our study, there was no association between the Bsm1 polymorphism and diabetic macrovascular complications especially myocardiac infarction (Table 2).
These two contrary results (lower risk of retinopathy in B allele in our study, higher risk of coronary artery disease in B allele in other studies) may explained by biochemical features of Bsm1 polymorphism. Polymorphism for Bsm1 was known functional effects because it is located within intron 8 which will be removed during mRNA posttranscriptional. Although, VDR itself may not be the disease affecting locus, but rather a marker locus in linkage disequilibrium with the residual locus, and the discrepant findings may reflect variable strengths of linkage disequilibrium in different populations [15]. Another possible mechanism is that alternation of Bsm1 in intronic sequence may influence protein expression [14].
There are several hypotheses for development of metabolic disorder in alternation of vitamin D system. First, vitamin D is fat soluble and can be stored in adipose tissue. Second, large cohort studies have been reported that high BMI is strongly and inversely correlated with serum vitamin D level. Third, vitamin D regulates calcium trafficking in pancreatic β-cells in vitro. Also, vitamin D effects intracellular ionized calcium signaling in the adipocyte, which in turn induces increased lipogenesis and decreased lipolysis via uncoupling protein-2. These mechanisms postulated that alternation of the VDR potentially contributes to the development of metabolic syndrome and cardiovascular disease. Unfortunately, our patients have only few data with serum vitamin D level, so we couldn't evaluate the association with vitamin D level and other results.
In present study, we suggested that Bsm1 polymorphism in VDR gene is associated with lower risk of diabetic retinopathy in type 2 diabetic patients. Bsm1 polymorphism in VDR gene could be used as a susceptibility marker to predict the risk of diabetic complication. But further large study will be needed.

 XML Download
XML Download