

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Diabetic patients with similar mean glucose levels often exhibit differences in terms of both the number and degree of glucose excursions. This phenomenon, termed glucose variability, has been suggested as a factor associated with diabetic complications. The development of continuous glucose monitoring (CGM) systems has revolutionized the monitoring of short-term glucose variability, and understanding of the role of glucose fluctuations is in progress. Here, we provide an overview of the methods used to measure glucose variability and review the literatures on clinical implications associated with glucose variability.
GLUCOSE VARIABILITY MEASUREMENT
Table 1 describes the formulas underlying commonly used measurements and their characteristics. There is no generally accepted gold standard and little consensus regarding which method offers the most meaningful assessment of glucose variability. Among the most commonly used methods is the standard deviation (SD). It can be calculated from self-monitoring of blood glucose (SMBG) levels. Since CGM was available, the mean amplitude of glycemic excursions (MAGE) has been widely used, too.
To avoid distortions in variability due to glycemic exposure, calculations of glucose variability should be devoid of a time component: glucose excursion×time=glycemic exposure, but not variability. Similarly, the formula glucose excursion/time=slope is the rate of glucose change, but not its magnitude [1]. Unlike the integrated measurement of long-term glucose control provided by hemoglobin A1c (HbA1c), glycemic variability requires comprehensive assessment of glycemia. CGM systems provide a more accurate measure of glycemia than does SMBG; however, issues of reproducibility limit the utility of this approach [2].
Intraday variability
The simplest method of assessing intra-day variability of serum glucose is to calculate the SD or coefficient of variation (CV) of multiple SMBG readings taken over the course of a day. Usually 7-point glucose measures are used, although important fluctuations can be missed simply because they occur between two measurements (Fig. 1). Furthermore, it is difficult to obtain information on nocturnal glycemic patterns. CGM systems are able to overcome many of the issues with SMBG glucose curves, though the data are still not normally distributed, a condition necessary for calculating the SD. However, the SD correlates well with other variability measures and is the only measurement identified to date where a relationship between glucose variability and mortality in intensive care unit can be demonstrated [34]. For these reasons, some groups have suggested the SD as the preferred method for assessing intraday glucose variability [5].
MAGE was originally developed using hourly glucose samples taken from venous blood [6], and it has emerged as the preferred method for assessing CGM data. In the example presented in Fig. 2, 1 SD of the mean glucose level for each 24-hour period acts as an individualized standard; only one limb of the excursion >1 SD, either ascending or descending, is used to calculate subsequent excursions. The arithmetic mean of these glycemic excursions over the period of study (24 hours or longer) is then used to calculate the MAGE; an automated algorithm has been created for this calculation [7]. Using this method, the mean glucose value becomes the reference point for glycemic variability. However, because the MAGE represents only major excursions from the mean and ignores excursions of <1 SD, this approach disregards smaller excursions that may be important.
The M-value was developed to quantify glycemic control of patients with type 1 diabetes mellitus (T1DM) using a reference value of six blood sugar measurements taken over a 24-hour period [8]. This approach measures the stability of glucose excursions relative to a user-defined "ideal" value ranging from 80 to 120 mg/dL. As a result, differences in user-defined "ideal" values have limited the ability to compare results between studies. In addition, M-values rise in response to increasing glycemic variability and poor glycemic control, making it difficult to distinguish between patients with high mean glucose levels and high glucose variability. Because hypoglycemia has a greater impact on the M-value than does hyperglycemia, this method is more relevant as a clinical, rather than a mathematical, indicator of glycemic control. A similar index which takes into account both the mean glucose level and variability of glycemia is the J-index [9].
In 1999, a new method, continuous overall net glycemic action (CONGA)-n, was developed specifically for use with CGM data [10]. This method calculates the difference between current glucose levels and that of glucose levels n hours previously, with n varying from 1 to 8 hours; readouts are then calculated using the SD of these differences. Because CONGA does not require arbitrarily defined glucose cutoffs or changes in glucose levels, this approach provides an objective assessment of glycemic variability over short time intervals. However, glucose differences are not normally distributed, limiting the applicability of this approach. Furthermore, which time segments produce the most useful results has yet to be determined.
Outside of measuring glucose itself, serum 1,5-anhydroglucitol (1,5-AG) levels have been suggested as a means of assessing glycemic excursions [11]. 1,5-AG is a polyol maintained within stable limits in subjects with healthy glucose levels. Its reabsorption in the kidney is inhibited by excessive excretion of urinary glucose; the higher the plasma glucose concentration, the lower the concentration of plasma 1,5-AG [12]. Urinary glucose only appears at plasma glucose concentrations over 160 mg/dL; therefore, 1,5-AG level seems of little use in detecting glucose fluctuations below this range. In addition, because both chronic and intermittent hyperglycemia are characterized by low concentrations of 1,5-AG, the correlation between glucose variability and 1,5-AG is poor when mean glucose levels remain high persistently. Use of the 1,5-AG concentration as a clinical marker is therefore limited to patients with postprandial hyperglycemia with HbA1c levels below 8% [1314]. Even though, 1,5-AG is not able to provide a direct measurement of glucose fluctuations, limiting the ability of this method to measure both the size and frequency of glycemic excursions.
Interday variability
The easiest way to measure interday variability of serum glucose is by calculating the SD of the fasting blood glucose concentration [15]. The absolute mean of daily differences (MODD) using hourly blood sampling was developed as a supplement to MAGE and mean blood glucose testing; this approach calculates the mean absolute value of the differences between glucose values on two consecutive days at the same time [16]. However, the timing of meals can greatly affect MODD scores, making a strict dietary regimen essential for accurate monitoring.
CONTRIBUTION OF GLUCOSE VARIABILITY TO CHRONIC COMPLICATIONS
It has been suggested that glucose variability may have been responsible for differences in microvascular outcomes between intensively and conventionally treated T1DM patients with the same mean HbA1c in the Diabetes Control and Complications Trial (DCCT) [17]. Although this hypothesis has since been refuted by the study authors themselves [18], interest in the relationship between glucose variability and chronic complications of diabetes has persisted. This interest has yet to progress to the point of randomized clinical trials, making the connection between these two factors largely speculative.
Hyperglycemia is thought to induce oxidative stress, which has been shown to exacerbate diabetic complications through a variety of molecular mechanisms [19]. The proposed contribution of glucose variability is supported by reports that oxidative stress is greater for intermittent as opposed to sustained hyperglycemia [202122], though contradictory evidence has also been reported [132324].
Microvascular complications
In the case of T1DM, a large proportion of studies have been secondary analyses of either the DCCT or the follow-up Epidemiology of Diabetes Interventions and Complications (EDIC) study. In these studies, the SD of SMBG results revealed no relationship between glucose variability and the risk of development or progression of microvascular complications (retinopathy and/or nephropathy) [18252627]. Glucose variability did not contribute to the development of neuropathy, although neuropathy data were more limited than other clinical covariates [28]. However, according to a prospective observational study that followed 100 patients with T1DM for 11 years, the SD of SMBG was found to be significantly related only with peripheral neuropathy and a borderline predictor of incidence (hazard ratio, 1.73; P=0.07) [29]. Therefore, these data suggest that the nervous system may be particularly vulnerable to glycemic variability. However, these studies relied on SMBG data, which may miss fluctuations occurring between the measurements.
A similar study assessing glycemic variability in T1DM patients using both CGM and SMBG readings revealed a strong correlation between microvascular complications and higher glycemic variability by CGM, but not by SMBG [30]. However, reproducibility remains an issue, with a conflicting report demonstrating no significant association between retinopathy and measures of glucose variability using CGM data in either T1DM or type 2 diabetes mellitus (T2DM) [31]. More studies are therefore necessary to determine the relationship between intraday glycemic variability and microvascular complications. In the meantime, long-term fluctuations such as HbA1c variability and the CV/SD of fasting blood glucose have been implicated in the development of retinopathy or nephropathy in T1DM [32] and T2DM [3334] by retrospective analyses. However, even these associations remain controversial [35].
Macrovascular complications
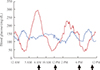
In terms of the DCCT study, the SD was not a predictor of cardiovascular events in patients with T1DM [36]. As for T2DM, some evidence of long-term variability in fasting plasma glucose as a prognostic factor for cardiovascular mortality has been seen in elderly patients [37]. Recent 7-point glucose data from the HEART2D study comparing basal insulin and prandial insulin after acute myocardial infarction (Fig. 3) reported no association between the mean absolute glucose (MAG), an intraday assessment of glucose variability, and the endpoint of combined cardiovascular events [38]. Because neither SD nor MAGE was significantly different between the two treatment groups, this interpretation has been challenged in part due to the reliance on MAG, with no other methods used to assess variability [39]. In the meanwhile, in patients with acute myocardial infarction, MAGE from CGM data collected at the time of admission independently predicted major adverse cardiac events [4041]. A subsequent cross-sectional study also showed that short-term glucose variability, as determined by CGM, was associated with the severity of coronary artery disease [42]. When we look at studies of surrogate endpoints such as subclinical atherosclerosis, more supportive evidence for associations with glucose variability can be found both in T1DM and T2DM [43444546]. However, a substantial proportion of the T2DM studies included mixed populations of patients treated with diet alone, diet and oral antidiabetic medications, and insulin. As such, this may have been a confounding factor in many of the findings, requiring further subgroup analyses to more accurately assess risk factors in this population.
CONCLUSIONS
While the data remain very heterogeneous, some conclusions can be drawn from this literature review. First, in the absence of a true gold standard for determining glucose variability, MAGE and SD have become the go-to methods for variability testing. CGM systems appear to be preferable to SMBG for capturing variability because of the larger number of data points possible with this approach. Second, little supporting evidence linking short-term glucose variability and microvascular complications exists, with full confirmation requiring use of a CGM system, particularly in patients with T1DM. The bulk of the T1DM data were derived from a single study (DCCT), limiting the generalizability of some conclusions; further studies are necessary to determine whether these findings are consistent across different populations. Prospective analyses examining the effects of long-term variability on microvascular complications are also needed. As for macrovascular complications, although the HEART2D trial suggested that lowering glucose variability does not improve cardiovascular outcomes in T2DM patients after acute myocardial infarction, subsequent studies demonstrated that glycemic variability has a probability of accelerating coronary artery disease in high-risk patients with T2DM. Large-scale randomized controlled trials are necessary to establish such a risk.










 XML Download
XML Download