

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Diabetes mellitus is a leading cause of mortality and increased disability-adjusted life years (DALYs) worldwide. In 2010, an estimated 1.3 million diabetes-related deaths occurred worldwide, which was twice as many as occurred in 1990 [1]. Furthermore, the DALYs from diabetes increased by 30% during this same period from 380 per 1,000 persons to 523 per 1,000 persons [2]. Although the mortality rate of diabetes in Korea decreased from 25.0 per 100,000 persons in 2003 to 21.5 per 100,000 persons in 2013, diabetes was still ranked as the fifth most common cause of death in 2013 [3]. In addition to its association with mortality, diabetes, and diabetes-related chronic complications such as retinopathy, neuropathy, nephropathy, cardiovascular, and cerebrovascular diseases, peripheral artery occlusive diseases, and amputations are related to significant increases in medical costs [4].
PREVALENCE OF DIABETES AND OBESITY
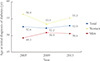
Recently, the prevalence of diabetes has increased in conjunction with the incidence of obesity. According the Korea National Health and Nutrition Examination Survey (KNHANES) studies in 2001 to 2013, the age-standardized prevalence of diabetes among adults 30 years of age and older increased from 8.6% to 11.0% and the age-standardized prevalence of adult obesity, defined as a body mass index (BMI) of 25 kg/m2 or higher, increased from 29.2% to 31.8% [56]. During the same period, the rates of diabetes and obesity tended to increase among men, while among women the prevalence of diabetes increased but the prevalence of obesity decreased (Fig. 1).
Studies have consistently reported an association between obesity and diabetes. In a large representative sample from the United States, the highest prevalence of diabetes was observed in subjects with a BMI ≥40 kg/m2 [7], and Menke et al. [8] found that changes in BMI over time are the greatest contributor to the increased prevalence of diabetes in this population. Eckel et al. [9] demonstrated that obesity is linked to diabetes through the increased production of adipokines and cytokines, reductions in adiponectin levels, altered ectopic fat deposition, and mitochondrial dysfunction. However, because not all obese individuals develop diabetes, the relationship between obesity and diabetes remains unclear. For example, the influence of abdominal obesity on the risk of diabetes was found to be more important than that of general obesity [10]. Given the striking parallel increases in the incidences of these two conditions, obesity is likely an important contributing factor to the manifestation of diabetes and the complications, mortality, and morbidity related to this disease [11].
In recent decades, there has been a dramatic increase in the number of obese people with diabetes in Korea. The average BMI of diabetic Korean patients increased from 21.9 kg/m2 in 1989 to 1990 to 24.8 kg/m2 in 2010 to 2012 [1213]. In 2013, 71.6% of men and 74.2% of women with diabetes were obese or overweight (Fig. 2, unpublished data).
AGE-SPECIFIC TRENDS IN THE PREVALENCE OF DIABETES
National surveys conducted between 2001 and 2013 in Korea revealed age-related increases in the prevalence of diabetes in all age groups, except for those between 30 and 39 years of age [5]. Because Korea is a rapidly aging society, this increase was particularly evident in people aged 70 years and older; the rate of diabetes in this age group was 27.6% in 2013, approximately twice as high as in 2001 (Fig. 3). However, the mean age at first diagnosis of diabetes was very similar among men in 2005 (49.3 years) and 2013 (50.6 years), while the mean age among women decreased slightly from 56.4 to 55.3 years (Fig. 4, unpublished data). Thus, there is roughly a 5-year difference between men and women in terms of age at the first diagnosis of diabetes.
According to the Centers for Disease Control and Prevention in the United States, the mean and median ages at the first diagnosis of diabetes among American adults aged 18 years or older were 53.7 and 53.8 years in 1997 and 53.8 and 54.2 years in 2011 [14]. The median ages at diagnosis of diabetes were 53.6 years for men and 55.2 years for women in 2011 [14]. In Korea, the age at the diagnosis of diabetes is similar to that in the United States, but Korean men tend to develop diabetes about 3 years earlier than American men (unpublished data).
OBESITY AND AGE AT THE DIAGNOSIS OF DIABETES
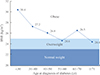
The KNHANES 2013 revealed an inverse linear relationship between BMI and age at diagnosis of diabetes among newly diagnosed subjects (Fig. 5, unpublished data). It has been reported that obesity is independently associated with early onset diabetes [15] and the European Prospective Investigation into Cancer and Nutrition-Potsdam Study found that weight gain in early adulthood (25 to 40 years) is more strongly associated with the risk and earlier onset of diabetes than weight gain after the age of 40 years [16].
A number of studies have reported that the age at onset and duration of diabetes are associated with microvascular events, cardiovascular disease, and all-cause mortality. For example, Banerjee et al. [17] suggested that the duration of diabetes is an important determinant of ischemic stroke risk. Zoungas et al. [18] reported that diabetes duration is independently associated with the risk of macrovascular complications such as cardiovascular death, non-fatal myocardial infarctions or nonfatal strokes, microvascular complications such as nephropathy and retinopathy, and death from any cause. Additionally, a longer duration of diabetes is associated with serious diabetes-related long-term complications in midlife [19].
Wannamethee et al. [20] demonstrated that people who developed diabetes prior to 60 years of age had a risk of coronary heart disease that was approximately twice that of persons who were diagnosed with diabetes after age 60. Because the chronic worsening of hyperglycemia is generally associated with an insulin insufficiency in individuals with a longer duration of diabetes, it is difficult to determine the underlying mechanisms. This finding may have important public health and economic implications because individuals with diabetes tend to require sustained health services and often develop early complications during the period of highest productivity.
CONCLUSIONS
In conclusion, the prevalence of diabetes is increasingly shifting to younger individuals and obese people. As more people develop diabetes earlier and live longer, public efforts should focus on healthy lifestyle changes, primary prevention measures, screening for the early detection of diabetes, and long-term management. Following a diagnosis of diabetes, treatment measures should include intensive glycemic control to minimize the risk of microvascular and macrovascular complications. Because the treatment of obesity is an important intervention that can reduce the prevalence of diabetes, the management of obesity should be considered for obese people with diabetes.



 XML Download
XML Download