

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Celiac disease is a chronic autoimmune disorder of the small intestine with a morbidity that has increased rapidly over the past 30 to 40 years [1]. According to a recent study, the prevalence of this disease is ~1% in Europe and USA, but it has not yet been reported in Korea [2]. In the disease process, genetically susceptible individuals are exposed to prolamins following the ingestion of certain grains, such as wheat, barley, and rye. This triggers autoimmune responses in the intestinal mucosa, resulting in chronic inflammation and villous atrophy in the small intestine. This, in turn, leads to nutritional malabsorption [3]. That is, celiac disease occurs through an interaction between environmental and genetic factors.
The main genetic factors include the HLA-DQ2 and DQ8 gene loci of human leukocyte antigen (HLA) class II genes [4]. Indeed, ~90% of patients with celiac disease carry HLA-DQ2 heterodimers ("DQ2.5"), encoded by the HLA-DQA1*05 and HLA-DQB1*02 alleles [5]. The remaining patients (~5% to 10%), who are DQ2.5-negative, nearly all carry HLA-DQ8 heterodimers ("DQ8"), encoded by the HLA-DQB1*03:02 allele, generally in combination with the HLA-DQA1*03 variant [5,6,7].
A 47-year-old woman complained of persistent chronic diarrhea and weight loss over the previous 9 months. The patient was diagnosed with celiac disease and was found to be genetically predisposed, due to HLA-DQ2.5, and had coexisting Graves' disease. To our knowledge, this is only the second reported case of celiac disease coexisting with Graves' disease diagnosed in Asia and the first case in Korea. Here, we report this case along with a review of the literature.
CASE REPORT
A 47-year-old woman was referred to our hospital due to watery diarrhea with weight loss. The patient had up to 20 episodes of watery diarrhea daily and a 15-kg weight loss over the previous 9 months. Thyroid function tests showed increased levels of triiodothyronine (221 ng/dL; normal range, 80 to 200 ng/dL) and free thyroxine (FT4; 3.51 ng/dL; normal range, 0.77 to 1.94 ng/dL) and decreased levels of thyroid stimulating hormone (TSH; 0.05 µIU/mL; normal range, 0.30 to 4.00 µIU/mL). Additionally, a thyroid autoantibody test showed increased levels of anti-thyroid peroxidase antibody (2,162 IU/mL; normal range, 0 to 8 IU/mL), anti-thyroglobulin antibody (166.4 IU/mL; normal range, 0 to 60 IU/mL), and TSH-binding inhibitory immunoglobulin (27.7%; normal range, 0% to 10%). Thyroid ultrasound revealed diffuse low echogenicity and increased blood flow on color Doppler.
Accordingly, she was diagnosed with Graves' disease and subsequently treated with methimazole. After 6 months of treatment, thyroid function tests showed normal levels of FT4 (1.3 ng/dL) and TSH (0.37 µIU/mL), but the patient still complained of persistent watery diarrhea and abdominal distension. A weight gain of 6 kg had been achieved in the 2 weeks following the initiation of treatment, but no further weight recovery was achieved.
She was admitted to the hospital to determine the cause of her persistent symptoms. Physical examination showed the patient had a height of 161 cm, weight of 60 kg, blood pressure of 124/67 mm Hg, pulse of 87 beats per minute, respiratory rate of 18 breaths per minute, and body temperature of 36.3℃. The patient had no abdominal pain, tenderness, or edema. Laboratory results were within normal limits. White blood cells (WBCs; 8,250/µL; normal range, 4,000 to 10,000/µL), hemoglobin (13.3 g/dL; normal range, 12 to 16 g/dL), platelet count (279,000/µL; normal range, 150,000 to 350,000/µL), sodium (139 mmol/L; normal range, 135 to 145 mmol/L), potassium (3.6 mmol/L; normal range, 3.5 to 5.0 mmol/L), total protein (6.6 g/dL; normal range, 5.8 to 8.0 g/dL), albumin (4.1 g/dL; normal range, 3.1 to 5.2 g/dL), cholesterol (126 mg/dL; normal range, <200 mg/dL), alkaline phosphatase (62 IU/L; normal range, 50 to 128 IU/L), aspartate aminotransferase (19 IU/L; normal range, <40 IU/L), and alanine transaminase (22 IU/L; normal range, <40 IU/L) were all normal. Stool lipid testing was found to be normal. No WBCs were observed in the stool examination, and no bacterial growth was identified in the stool culture. In addition, the patient showed negative results for detection of the antihuman immunodeficiency virus antibody and antinuclear antibody testing.
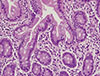
Abdominal computed tomography scan showed no ascites or enlarged lymph nodes, and no edema or masses were observed in the small intestine (Fig. 1). Esophagogastroduodenoscopy showed no abnormal findings in the duodenal bulb (Fig. 2). Colonoscopy showed no gross abnormal finding in the colonic mucosa. The patient also underwent 'random' biopsies. A random biopsy of the colon showed normal variation. A duodenal bulb biopsy showed no significant villous atrophy, but a slight increase in intraepithelial lymphocytes was seen (Fig. 3).
Based on the medical history of Graves' disease, persistent chronic diarrhea with weight loss, and increased intraepithelial lymphocytes of the patient, she was suspected to have celiac disease. Accordingly, the patient was placed on a gluten-free diet and subjected to serological and genetic tests.
As a result of HLA typing, HLA-DQA1*03 and *05 and HLA-DQB1*02:01 and *04:01 were detected in the patient. Thus, the patient had an HLA-DQ2 heterodimer ("DQ2.5") comprising HLA-DQB1*02:01 and HLA DQA1*05. Megiorni and Pizzuti [5] reported that DQ2.5 is a high-risk factor for celiac disease. Serological analysis showed that the patient did not have immunoglobulin A (IgA) anti-tissue transglutaminase (anti-tTG) or IgA endomysial antibodies.
Diarrhea was reduced from 20 times to 0 to 1 time per day starting from the second day of the gluten-free diet. At 4 weeks after initiating the gluten-free diet, the patient's weight had increased by 8 kg, reaching 68 kg, and her clinical symptoms had also improved. During a 6-month follow-up, diarrhea recurred only twice after consuming noodles containing gluten.
The patient is currently maintaining a gluten-free diet. Although serologic testing was negative, the patient was finally diagnosed with celiac disease after identifying the HLA-DQ2.5 genotype and the diagnosis of Graves' disease.
DISCUSSION
Indications considered in the diagnosis of celiac disease occur in three tiers: first, typical symptoms, such as chronic diarrhea, malabsorption, weight loss, and abdominal distension; second, unexplained iron deficiency anemia, folate, or vitamin B12 deficiency, elevation of serum aminotransferase, delayed puberty, decreased reproductive function, aphthous ulcers, peripheral neuropathy, recurrent migraine, and cerebellar ataxia; and third, membership of a patient group with a high risk of celiac disease [8]. Such high-risk groups include those with type 1 diabetes, other autoimmune diseases, familial history of celiac disease, Turner syndrome, Down syndrome, or Williams syndrome [8,9]. In this case, celiac disease was suspected because the patient showed typical symptoms and had a previously diagnosed autoimmune disease.
All examinations to diagnose celiac disease should be conducted while patients are following a gluten-containing diet. Furthermore, celiac disease cannot be diagnosed via a single examination. For the diagnosis of celiac disease, symptoms such as diarrhea and malabsorption, serological findings of anti-tTG and IgA endomysial antibodies, villous atrophy of the small intestine on duodenal biopsy, elevation of intraepithelial lymphocytes, HLA typing, and clinical improvement after beginning a gluten-free diet should be considered together. Megiorni et al. [10] classified the risk gradient of celiac disease according to HLA-DQ typing, in that patients with DQ2.5 or DQ8 were considered to be a very high-risk group.
In this case, a middle-aged female patient with previous complaints of chronic diarrhea was diagnosed initially with Graves' disease. However, subsequent treatment did not lead to resolution of all symptoms. Finally, she was diagnosed with celiac disease and the HLA-DQ2.5 genetic predisposition in addition to Graves' disease. The diagnosis of celiac disease was based on increased intraepithelial lymphocytes, DQ2.5 positivity, and the response to a gluten-free diet.
Based on recent studies and reviews [11,12], even though celiac disease originally was considered a rare malabsorption syndrome of childhood, affecting mainly Caucasians, it is now recognized as a more common condition that may affect many races and ethnic groups at almost any stage of life. Green and Cellier [11] reported the mean age at diagnosis was 46.4±1.0 years (range, 16 to 82). Also, its clinical presentation varies widely, ranging from classical gastrointestinal manifestations to only atypical signs [13]. Many cases remain undiagnosed or are not diagnosed until later because of the wide variability in symptoms. In our case, the severe gastrointestinal symptoms of celiac disease presented in late adulthood and were accompanied by Graves' disease, even if there might have been a prior latent period. The diagnosis of celiac disease was delayed for 14 months because of the coexistence with Graves' disease and a lack of suspicion due to the low incidence of celiac disease in Koreans.
A case of celiac disease coexisting with Graves' disease is rare in Asia. To our knowledge, this is only the second reported case in Asia and the first in Korea. A case of combined primary hyperparathyroidism, Graves' disease, and celiac disease was reported previously in Lebanon [14]. There was only one previous domestic case report of celiac disease, but with no coexisting autoimmune diseases [15]. A few cases in Europe and Canada include adult patients with Graves' disease diagnosed with celiac disease due to chronic diarrhea, malabsorption, or bone deformities [16,17,18]. The case presented here differed from these other cases in that two autoimmune diseases were diagnosed in a patient who had no previous disease history and who was positive for DQ2.5 by HLA typing.
Although the patient belonged to a very high-risk group for celiac disease, due to typical symptoms and DQ2.5 positivity, serological tests were negative, despite their high sensitivity and specificity. The reason for the negative serological tests is likely attributable to the timing of the serological tests, which were conducted after the gluten-free diet was initiated; however, all examinations should be conducted while a patient is eating a gluten-containing diet. In such a case, a gluten tolerance test may be performed for a more accurate diagnosis [19]. If the result of a duodenal biopsy is positive after consuming 3 g gluten daily for 2 weeks, or if the result of a serological test is positive after a 6 week gluten-containing diet, the patient is diagnosed with celiac disease [19]. In this case, however, a gluten tolerance test was not conducted because of the pain caused by the symptoms and economic reasons. According to a recent study, HLA genotyping is a useful diagnostic method for celiac disease in patients treated with a gluten-free diet without a confirmatory diagnosis [20].
In conclusion, celiac disease was diagnosed clinically in a patient with HLA-DQ2.5 and Graves' disease. This is the first case of celiac disease coexisting with Graves' disease reported in Korea. Further, this case is meaningful in that HLA genotyping showed DQ2.5 positivity, a high-risk factor for celiac disease. Celiac disease is relatively common in Europe and USA. However, due to changes in dietary patterns and the development of better diagnostic methods, the prevalence of celiac disease is expected to increase in Asian patients with prior autoimmune diseases.

 XML Download
XML Download