

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Malignant neoplasms, cerebrovascular disease, heart disease, and diabetes have been the major causes of mortality in Korea over the last 10 years [1]. All of these are closely related to an obesity epidemic. The body mass index (BMI) is the most widely used method for the diagnosis of obesity and is correlated directly with the risk of comorbidities and mortality. Evidence from epidemiological studies has demonstrated the importance of body fat distribution and the strong association of excess abdominal fat with insulin resistance, dyslipidemia, hypertension, and diabetes, and their essential roles in the pathogenesis of cardiovascular disease, metabolic syndrome, and certain cancers. However, BMI has important limitations, because it neither discriminates fat from lean mass nor fully reflects the distribution of body fat. Waist circumference (WC) has been commonly used as a simple and clinically useful surrogate marker for central adiposity. The determination of WC cutoff values is important in the prevention and treatment of obesity, type 2 diabetes, and related cardiovascular diseases.
This review focused on the current WC cutoff levels used in different ethnic groups and Koreans and suggested optimal WC cutoff values to identify abdominal obesity and predict disease risk in Koreans based on the analysis of large cohort data.
CURRENT THRESHOLDS FOR ABDOMINAL OBESITY IN DIFFERENT POPULATIONS/ETHNIC GROUPS
Abdominal obesity is highly correlated to insulin resistance. Because abdominal obesity was a major component of metabolic syndrome in the National Cholesterol Education Program Adult Treatment Panel III (NCEP ATP III) [2], the determination of the WC cutoff level to identify abdominal obesity has been performed by numerous organizations [3,4,5,6,7,8,9,10,11,12]. In the 2001 NCEP ATP III guidelines, abdominal obesity was defined as a WC ≥102 cm in males and ≥88 cm in females [3,13]. However, these cutoffs corresponded to BMI values of 30 kg/m2 based on studies performed in populations of European origin [14].
The International Diabetes Federation consensus proposed ethnicity-specific WC cutoff values, which have been incorporated into the definition of metabolic syndrome [15,16]. Likewise, the 2005 revised NCEP criteria proposed by the American Heart Association/National Heart, Lung, and Blood Institute [4] indicated a minor lowering of the WC cutoff levels to ≥90 and ≥80 cm in males and females, respectively, which appeared to be appropriate for Asian Americans.
WC thresholds for abdominal obesity are not uniformly applicable to all populations and ethnic groups, because variations in disease risk may occur with the same WC in different ethnic groups. The 2009 joint statement harmonizing metabolic syndrome recommended the use of ethnicity-specific WC thresholds. Table 1 lists WC thresholds recommended for different populations and ethnic groups.
CHANGES IN WC CUTOFF LEVELS FOR ABDOMINAL OBESITY IN THE KOREAN POPULATION
Until 2005, WC thresholds of ≥90 cm (36 inches) in males and ≥80 cm (32 inches) in females were used as the diagnostic criteria for abdominal obesity in Korea. These were determined from results that obesity-related disorders may begin to increase rapidly from a WC of 90 to 92 cm (36 inches) in males and from 80 to 82 cm (30 inches) in females. These were in accordance with the definition from the 2000 Western Pacific Region of the World Health Organization, International Association for the Study of Obesity, and International Obesity Taskforce guidelines based on epidemiological data from Chinese living in Hong Kong and Singapore [5]. These criteria raised several issues, and re-evaluation of the threshold for abdominal obesity criteria was required. In brief, the cutoff level of 80 cm in females was considered to be low and very near to the mean WC of 78.31 cm according to the 1998 National Health and Nutrition Examination Survey of Korean females. Furthermore, the 40.3% prevalence of obesity in females was relatively high compared with the 19.9% morbidity in males [17].
In 2006, the Korea Society for the Study of Obesity updated the WC cutoff levels for defining abdominal obesity to 90 cm in males and 85 cm in females [18]. These cutoffs were defined by receiver operating characteristics (ROC) curve analysis, odds ratios, and the prevalence of abdominal obesity based on representative sample data from the 1998 Korean National Health and Nutrition Examination Survey [18]. The WC cutoff levels in Koreans using ROC curve analysis for two or more metabolic syndrome risk factors as a reference were 82 to 84 cm in males and 79 to 82 cm in females. The odds ratio of having more than two metabolic abnormalities was approximately 5 in males and females with a WC ≥90 and ≥80 cm, respectively. WC values in the 80th percentile in the Korean population were 90 and 86.5 cm in males and females, respectively.
There have been numerous studies attempting to identify the optimal WC cutoff in the Korean population since 2006 [19,20,21,22,23,24,25,26,27,28,29]. Table 2 shows those studies that proposed thresholds for abdominal obesity in Koreans [19,20,21,22,23,24,25,26,27,29]. The range of optimal WC cutoffs were determined to be 80 to 89.8 cm in males and 76.1 to 86.5 cm in females. However, most studies were cross-sectional in design [19,20,22,23,24,26,27,28,29], which have an inherent shortcoming potentially leading to incorrect conclusions regarding the relationship between obesity and disease. Further prospective studies using representative populations, common health outcomes, and proper analytical approaches are needed to identify optimal cutoff levels.
OPTIMAL WC CUTOFF LEVELS TO IDENTIFY ABDOMINAL OBESITY USING THE ANSUNG-ANSAN AND NATIONAL HEALTH INSURANCE CORPORATION COHORTS
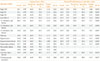
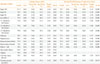
We analyzed the data from two large cohorts using ROC curve analysis to maximize the sensitivity and specificity for identifying optimal WC cutoff levels and to overcome the limitations of a cross-sectional design. The outcome variables were incidence of diabetes, hypertension, dyslipidemia, cerebrovascular disease, myocardial infarct, angina, coronary artery disease, and multiple metabolic risk factors. Tables 3, 4 show the area under the curve and optimal cutoff levels with corresponding validity parameters for WC in predicting different types of obesity-related diseases in males and females, respectively.
Among males, the optimal WC cutoff points identifying the presence of two or more metabolic risk factors were 80.3 and 80.5 cm in the Ansung-Ansan and National Health Insurance Corporation (NHIC) cohorts, respectively. The optimal cutoff values for identifying the incidence of diabetes, hypertension, hypercholesterolemia, and hypertriglyceridemia were 84.0, 83.8, 83.2, and 82.7 cm, respectively, in the Ansung-Ansan cohort. These results were similar to those from the NHIC cohort. An area under the curve value of 0.66 for a WC of 90 cm identified myocardial infarction with a corresponding 52% sensitivity and 79% specificity. The optimal cutoffs for identifying coronary artery disease and cardiovascular accident (CVA) were 83.3 and 84.6 cm, respectively, in the Ansung-Ansan cohort, and 85.5 and 83.5 cm, respectively, in the NHIC cohort. Among females, the optimal cutoff values for predicting various types of obesity-related diseases, including high levels of fasting blood glucose, high blood pressure, high triglyceride, and low high density lipoprotein cholesterol, and at least one, two, or three metabolic risk factors, diabetes, hypertension, hypercholesterolemia, hypertriglyceridemia, angina, and coronary artery disease, ranged from 73.4 to 81.7 cm in the Ansung-Ansan cohort and 73.5 to 77.5 cm in the NHIC cohort. These values were approximately 5 cm less than those in males. According to the Ansung-Ansan cohort, the optimal cutoff levels for myocardial infarct and CVA (84.9 and 85.9 cm, respectively) were higher than those used to predict other diseases. Based on the above results, the optimal cutoff values for diagnosing abdominal obesity in males and females were approximately 85 and 80 cm, respectively.
We performed a Cox proportional hazard analysis to calculate the hazard ratio (HR) for having metabolic risk factors or an incidence of diabetes for different WC cutoff values. Fig. 1 shows the HRs for the incidences of one, two, three, or more metabolic risk factors and for the incidence of diabetes for a 5-cm increase in the WC according to the Ansung-Ansan cohort. The risks of having one, two, three, or more metabolic risk factors were significantly increased with increasing WC. The HRs and 95% confidence intervals (CI) from the lowest to the highest 5-cm interval WC category (5-cm interval category from <70 to ≥100 cm) for males were 0.88, 1.00, 1.46, 1.90, 2.34, 2.81, 2.76, and 2.95, respectively, (95% CI, 2.24 to 3.88) for the development of one or more metabolic risk factors; 0.73, 1.00, 1.67, 2.35, 3.15, 4.23, 4.66, and 5.16, respectively, (95% CI, 3.78 to 7.04) for the development of two or more metabolic risk factors; and 0.83, 1.00, 3.31, 5.04, 7.44, 10.76, 13.50, and 12.81, respectively, (95% CI, 7.65 to 21.45) for the development of three or more metabolic risk factors (all P<0.001 for trend). Females displayed similar HR trends for the development of one, two, three, or more metabolic risk factors. The HRs for the incidence of diabetes were significantly increased from WC cutoff values of ≥85 cm for males (HR, 1.89; 95% CI, 1.32 to 2.70; P<0.001) and ≥80 cm for females (HR, 1.89; 95% CI, 1.37 to 2.60; P<0.001).
The prevalence of abdominal obesity varied depending on the selected WC cutoff values (Table 5). According to the Korea National Health and Nutrition Examination IV data, the prevalence of abdominal obesity was 46.3% when a WC cutoff ≥85 cm was used to diagnose abdominal obesity in males and 41.6% when a WC cutoff ≥80 cm was used in females (Table 5). It is of interest that ≥60% of females aged ≥50 years were abdominally obese when 80 cm was applied as the WC cutoff level. Otherwise, the prevalence of abdominal obesity was 25.4% in males and 25.0% in females when WC values of 90 and 85 cm, respectively, were applied for the definition of abdominal obesity.
CONCLUSIONS
The optimal WC cutoff value determined should be that which can identify populations at a predefined level of risk of future health problems consistently. The optimal WC cutoff levels were 85 cm in males and 80 cm in females, based on data from large prospective cohorts using various health outcomes. However, when considering the prevalence of abdominal obesity and the health costs for its prevention and management, WC of 90 cm in males and 85 cm in females are probably more appropriate thresholds for abdominal obesity.




 XML Download
XML Download