

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Cardiovascular disease (CVD) is a major clinical problem and the most common cause of morbidity and mortality in patients with chronic kidney disease (CKD) [1]. In CKD patients, the relative risk of mortality from CVD increases as the glomerular filtration rate (GFR) decreases [2]. There are many factors involved in the development of CVD in CKD, including hyperglycemia, hypertension, hyperlipidemia, inflammation, hypercoagulability, uremic toxins, and ectopic calcification [3].
Vascular calcification strongly correlates with CVD mortality and is a well-known pathophysiologic mechanism that explains the association between renal function and cardiovascular mortality [4]. Previous studies showed that renal dysfunction is associated with higher coronary artery calcium score (CACS) in predialysis and dialysis CKD patients [5,6], while in some studies the association between impaired renal function and coronary artery calcification (CAC) was not significant or was strongly attenuated after adjusting for cardiovascular risk factors [7]. A recent prospective study on data generated from the Multi-Ethnic Study of Atherosclerosis (MESA) revealed that the association between CKD and CAC is mediated through a characteristic elevation in triglyceride (TG)-rich lipoproteins [8]. However, no studies on this issue have been performed on a large scale in the Korean population.
The aim of this study was to analyze the relationship between renal function assessed by estimated glomerular filtration rate (eGFR) and CACS as detected by multi-detector computed tomography (MDCT) in apparently healthy Korean adults.
METHODS
Subjects
This cross-sectional study was a part of the Kangbuk Samsung Health Study, in which subjects participated in a medical health checkup program at the Health Promotion Center of Kangbuk Samsung Hospital, Sungkyunkwan University School of Medicine, Seoul, Korea. The purpose of the medical health checkup program is to promote the health of employees through regular medical checkups and to enhance early detection of existing diseases. Most of the examinees are employees and family members of various industrial companies from around the country.
The subjects participated in the medical checkup program from January 2010 to December 2011. We excluded subjects with a self-reported history of ischemic heart disease, ischemic stroke, subjects who were taking a statin or aspirin, and subjects with any missing data. Since few subjects had eGFR values lower than 60 mL/min/1.73 m2, subjects with eGFR <30 mL/min/1.73 m2 were excluded from the study. These rigorous exclusions resulted in a final study population of 23,617 subjects.
The participants provided written informed consent for the use of health screening data in this study. The design, protocol, and the consent procedure of this study were reviewed and approved by the Institutional Review Board of Kangbuk Samsung Hospital (KBS13120) and is in accordance with the Helsinki Declaration of 1975.
Anthropometric and laboratory measurements
Height and weight were measured twice and then averaged. The body mass index (BMI) was calculated by dividing the weight (kg) by the square of the height (m). Blood pressure (BP) was measured using a standardized sphygmomanometer after 5 minutes of rest.
Serum calcium level was measured using the O-cresolphthalein complexone method (Hitachi Modular D2400, Roche, Tokyo, Japan). The hexokinase method was used to test fasting glucose concentrations (Hitachi Modular D2400). Fasting insulin concentrations were determined by electrochemiluminescence immunoassay (Hitachi Modular E170, Roche). An enzymatic calorimetric test was used to measure the total cholesterol and TG concentrations. The selective inhibition method was used to measure the level of high density lipoprotein cholesterol (HDL-C), and a homogeneous enzymatic calorimetric test was used to measure the level of low-density lipoprotein cholesterol. Serum high-sensitivity C-reactive protein levels were measured using a nephelometric assay with a BNII nephelometer (Dade Behring, Deerfield, IL, USA).
The presence of diabetes mellitus was determined by answers to the participants' self-questionnaire and the diagnostic criteria of the American Diabetes Association [9]. The presence of hypertension was defined as BP ≥140/90 mm Hg or presently taking antihypertensive medication, according to the criteria recommended by the seventh report of the Joint National Committee on prevention, detection, evaluation, and treatment of high BP (JNC 7) [10].
Smoking status was determined by the answers to the self-questionnaire. A smoker was defined as a subject who had ever smoked at least five packs of cigarettes in his life. Doing exercise was defined as regular exercise of moderate intensity ate least three times a week. Insulin resistance was measured using the homeostatic model of the assessment of insulin resistance (HOMA-IR) and was obtained by applying the following formula: HOMA-IR=fasting insulin (IU/mL)×fasting blood glucose (mmol/L)/22.5 [11].
Assessment of renal function
eGFR was calculated using the Cockcroft-Gault equation: (140-age)×weight by kg×0.85 if female/(serum creatinine×72). Subjects were divided into three groups according to the CKD staging system with eGFR grade: stage 1, eGFR ≥90 mL/min/1.73 m2; stage 2, eGFR 60 to 89 mL/min/1.73 m2; and stage 3, eGFR 30 to 59 mL/min/1.73 m2 [12].
Assessment of CAC
MDCT for CACS was undertaken by a 64-slice, spiral computed tomography scan (GE Health Care, Tokyo, Japan). The severity of CAC was assessed by the Agatston score: 0, 1 to 10, 11 to 100, 101 to 400, or 400 [13]. A total CACS was determined by the sum of the individual scores for the four major epicardial coronary arteries. A significant CAC was defined as CACS >0.
Statistical analysis
Because the distribution of calcium scores was skewed, we used the logarithmic transformation of the calcium scores and added 1 to all calcium scores to deal with values of zero as previously analyzed (Ln [CAC+1]) [14]. Pearson's correlation analysis was used for bivariate correlation analyses between CACS+1, eGFR, and the variables of interest to more fully use the information contained in CACS. Comparison of the parameters between the subjects with or without CAC was analyzed by Student t test. Comparison of the parameters among the three groups divided by the stage of renal function was analyzed by a one-way analysis of variance. Binary logistic regression analyses were performed with other confounding variables included in the model. Significance was defined as P<0.05. All data were analyzed using SPSS version 18.0 (IBM Co., Armonk, NY, USA).
RESULTS
Study population
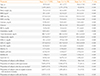
General characteristics of the participants are presented in Table 1. Mean age of the participants was 41.4 years (range, 23 to 89). The mean BMI value was 24.4 kg/m2, and 81.7% of the participants were male. Of the study population, 5.5% were being treated for diabetes or satisfied the diagnostic criteria for diabetes, 43.7% were hypertensive, and 33.3% had smoked more than five total packs of cigarettes in his or her life. Only 12.4% of the study population had significant CAC (CACS >0). Mean CACS significantly increased with age (data not shown). Compared with the subjects without calcification, the patients with calcification were older, were more obese with a higher BMI, and had higher systolic blood pressure (SBP) and diastolic BP. In addition, a greater number of these patients had a history of diabetes and hypertension (Table 2). Subjects with calcification had significantly lower eGFR values compared with subjects without calcification (104.1±21.6 vs. 99.9±21.9, P<0.01).
Correlation of CACS and eGFR with variable parameters
Bivariate correlation analyses were performed between CACS+1 and eGFR with multiple variables. Age showed the highest correlation with CACS+1 (r=0.327, P<0.01), and eGFR showed a slightly negative but significant association with CACS+1 (r=-0.076, P<0.01) (Table 3). Most of the parameters showed positive correlations with CACS+1 except HDL-C. Age showed a moderate negative correlation with eGFR (r=-0.419, P<0.01).
The relationship between renal function and coronary artery calcification
When mean CACS was compared among the CKD stages, the mean CACS significantly increased from stage 1 to 3 (stage 1, 0.33±1.0; stage 2, 0.47±1.3; and stage 3, 1.39±2.2; P<0.01) (Table 4). The proportion of subjects who had CAC significantly increased from stage 1 to 3 (stage 1, 11.2%; stage 2, 14.8%; and stage 3, 34.8%; P<0.01) (Fig. 1).
When logistic regression analysis was performed with CAC as the dependent variable, and after adjusting for dependent variables including SBP, glucose, total cholesterol, TG, BMI, and gender, the odds ratio (OR) for CACS was 1.99 (95% confidence interval [CI], 1.81 to 2.19; P<0.01) for the GFR stage 2 group and 8.58 (95% CI, 5.99 to 12.30; P<0.01) for the GFR stage 3 group, with the GFR stage 1 group being the reference group (Table 5). However, the OR significantly decreased from stage 1 to 3 when age was included in the model. Age was the strongest factor found to affect CAC.
DISCUSSION
In this study, renal function assessed by eGFR negatively correlated with coronary calcium score measured by MDCT based on data from Korean participants with normal to moderate renal dysfunction. When the subjects were divided into three groups according to the CKD staging system, the proportion of subjects with CAC significantly increased as kidney function deteriorated. In logistic regression analysis with CAC as the dependent variable, the OR for CAC increased as renal function deteriorated. However, these results were reversed when age was included in the model, suggesting that age was the strongest factor that affects CAC.
Several studies have revealed that age is the strongest factor for CAC. In a population-based study in older subjects, age, and male sex were the most important risk factors for coronary calcification. Newman et al. [15] examined CAC in an elderly cohort over the age of 65 years. The key findings of this study were that the extent of CAC was strongly associated with age through the ninth decade in men and women and was associated with CVD. However, the above-mentioned studies enrolled only elderly subjects and did not evaluate kidney function. The association between CAC and age in relatively healthy young subjects remains unclear.
Numerous risk factors have been reported for vascular calcification in CKD [16]. Some factors are traditional, including aging, hypertension, diabetes or dyslipidemia, and others are nontraditional, such as hyperphosphatemia, secondary hyperparathyroidism, low vitamin D, fibroblast growth factor 23, inflammation, and oxidative stress. Transformation of vascular smooth muscle cells into chondrocytes or osteoblast-like cells seems to be a key element in vascular calcification pathogenesis [17]. Is seems likely that medial calcification is the main phenotypic change in CKD, and the subsequent arterial stiffness, even in nondialyzing CKD patients, might lead to increased CVD in CKD patients [18]. Vascular calcification could be the mechanistic explanation for increased CVD mortality in CKD patients, since increased vascular calcification reflects increased total CVD burden [19].
Several epidemiological studies reported the association between decreasing kidney function and increased CAC. In the Dallas Heart Study, Kramer et al. [7] evaluated 2,660 participants with a median age of 49 and observed a strong association between CKD and CAC among diabetic participants. In contrast, in the Framingham Heart Study, Fox et al. [20] evaluated 319 subjects with nearly normal kidney function and observed an association between a lower eGFR and a higher prevalence of CAC in an unadjusted analysis, but the association was attenuated after multivariate adjustment for cardiovascular risk. Joosen et al. [21] investigated whether mild to moderate CKD is independently associated with coronary plaque burden beyond traditional cardiovascular risk factors. Although decreasing renal function was associated with increasing extent and severity of coronary artery disease, mild to moderate CKD was not independently associated with coronary plaque burden after adjustment for traditional cardiovascular risk factors. In the MESA study, a representative cohort study using the largest CACS database, there was an increasing CAC incidence risk ratio as the eGFR decreased. This phenomenon was attenuated after adjusting for elevated TG-rich lipoprotein lipid phenotype, suggesting the role of lipid abnormalities in the development of CAC in CKD patients [8]. In the Rotterdam study, El Barzouh et al. [14] evaluated 1,703 subjects with a median age of 70 years and observed that the association of CAC and GFR is affected by age. In our study, risk for CAC increased as renal function deteriorated from normal to moderate renal dysfunction. However, this significance disappeared as the model was adjusted for age, a result that is consistent with previous studies [14,20].
In another study performed on a Korean population, Cho et al. [22] evaluated the independent association between early CKD (stages 1 to 3a) with coronary atherosclerosis for 4,297 asymptomatic subjects. They showed that early CKD was an independent risk factor for coronary atherosclerosis, and the risk stratification for coronary atherosclerosis should be based on the presence of proteinuria rather than decreased eGFR within early CKD. Another study by Roy et al. [23] evaluated the relationship between CACS and stages of predialysis CKD and showed significantly increased risk for CAC compared with subjects with CKD. They suggested that mild and moderate predialysis CKD are independent risk factors for increased mean and incident CAC.
Our study had several limitations. First, this is a cross-sectional study; therefore, we cannot draw clear conclusions on the association of CKD and CAC from the results of our study. Second, we had no data on patient dietary intake of calcium, vitamin D, or magnesium, which may affect CACS. Third, we only used the Cockcroft-Gault equation to estimate eGFR. Recent work showed that GFR estimated by the Modification of Diet in Renal Disease study equation or Chronic Kidney Disease Epidemiology Collaboration equation overestimated GFR in stage 3 CKD when compared with the gold standard diethylene-triamine-pentaacetate method in the elderly [24]. Our study has strength in that we enrolled relatively healthy young subjects who participated in the medical health checkup program, and we showed that in this young population, age was the strongest factor that affects CAC as the kidney function declines.
In conclusion, age had the strongest effect on the association between eGFR and the degree of CAC in young Korean subjects with relatively normal renal function. In the future, prospective studies are needed to determine the relationship between CAC and the occurrence of overt CVD events. Also, further study is needed to determine whether early and intensive intervention of CKD patients with CAC can lead to improvement in rates of CVD morbidity and mortality.





 XML Download
XML Download