

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Albumin is one of the major proteins synthesized in the liver. Energy supply is a very important determinant for the normal physiology of albumin production [1]. Indeed, reduced serum albumin levels are observed in medical conditions associated with malnutrition [2-4], whereas high serum albumin levels have been reported to be associated with metabolic syndrome, an indicator of obesity and overnutrition [5]. In addition, recently, serum albumin has been suggested to be associated with insulin resistance [6].
In contrast, several studies reported that lower concentrations of serum albumin are associated with an increased risk of coronary heart disease, cardiovascular mortality, and carotid atherosclerosis [6,7]. Both the antioxidant and anti-inflammatory properties of albumin in the atherogenetic process have been suggested as possible mechanisms for this inverse association [6-10]. Considering that oxidative stress and chronic inflammation play crucial roles in the generation of both insulin resistance and type 2 diabetes [11,12], the antioxidant and anti-inflammatory properties of serum albumin may be associated with incident diabetes, as observed in the association with coronary heart disease, cardiovascular mortality, and carotid atherosclerosis.
Patients with nonalcoholic fatty liver disease (NAFLD) or impaired fasting glucose (IFG) are considered to be insulin resistant [13-15]. Homeostasis model assessment of insulin resistance (HOMA-IR) is a useful method for evaluating insulin resistance [16]. Thus, in the present study, we evaluated the association between serum albumin concentration and insulin resistance, as estimated by HOMA-IR and the presence of IFG and NAFLD. We also investigated whether serum albumin level had an independent effect on the development of diabetes.
METHODS
Study population
More than 80,000 people undergo a comprehensive heath check-up each year at Total Healthcare Center at Kangbuk Samsung Hospital. Most of those examinees get a medical check-up on their own initiative or are employees of various companies or their spouses largely paid for the cost by their employer to promote health; considerable proportions of them get a medical check-up annually or biannually. All data containing anthropometric information, laboratory tests, radiology imaging results and coded answers to self-reported questionnaires were stored electronically in medical records.
Our initial data was provided by 10,950 subjects who participated in comprehensive health check-ups annually for 5 years (between January 2005 and December 2009). Based on records from 2005, 1,921 subjects were excluded from the final analysis for the following reasons: 1) positive serologic markers for either hepatitis B (n=558) or C (n=17) virus; 2) liver cirrhosis (n=8); 3) white blood cell count >11,000/mm3 (n=98) or serum creatinine ≥1.5 mg/dL (n=45); 4) self-reported diabetes and undiagnosed diabetes fasting plasma glucose concentration ≥7.0 mmol/L or glycosylated hemoglobin (HbA1c) ≥6.5% (n=437); 5) malignancy (n=250); and 6) absence of data including HbA1c at any visit (n=632). Thus, final analyses were performed on 9,029 subjects (6,654 men and 2,375 women).
The informed consent requirement for this study was exempted by the Institutional Review Board because researchers only accessed the database for analysis purposes, and personal information was not accessed. This study was approved by the Institutional Review Board at Kangbuk Samsung Hospital.
Measurements
Serum albumin was measured by the Bromocresol green dye-binding method, using Bayer reagent packs on an automated chemistry analyzer (Advia 1650 Autoanalyzer, Bayer Diagnostics, Leverkusen, Germany). The intra-assay coefficient of variation was 1.3% and interassay coefficient of variation was 2.1%. Anthropometric variables, blood pressure (BP), and other biochemical markers were measured, as described previously [14]. Lifestyle information was self-reported.
Definitions
As a marker of insulin resistance, HOMA-IR was calculated using the following formula: HOMA-IR=[fasting insulin (µIU/mL)×fasting glycemia (mmol/L)]/22.5. Subjects with HOMA-IR level above the highest quartile (2.51 for men and 2.28 for women) were classified as having insulin resistance. IFG was defined as fasting plasma glucose between 100 and 125 mg/dL. Fatty liver was diagnosed using an abdominal ultrasonogram (Logic Q700 MR, GE, Milwaukee, WI, USA) based on known standard criteria, including hepatorenal echo contrast, liver brightness, deep attenuation, and vascular blurring. Several experienced radiologists performed the ultrasound exam. The development of diabetes was assessed from the annual records of all subjects and was defined as fasting plasma glucose ≥126 mg/dL or A1c ≥6.5%. In addition, based on the self-reported questionnaire at each visit, subjects who had a history of diabetes or who currently used insulin or other oral antidiabetic drugs were considered to have developed diabetes.
Statistical analysis
Results are expressed as the number of subjects with the percentage (%) and the mean value with standard deviation. One-way analysis of variance and Pearson's chi-squared test were used to analyze any statistical differences in study participant characteristics between tertiles of serum albumin. The odds ratio (OR) for the prevalence of insulin resistance (defined as the top quartile of HOMA-IR and the presence of IFG and NAFLD) was evaluated cross-sectionally according to the baseline albumin tertiles, using binary logistic regression. The hazard ratio (HR) for incident diabetes was estimated longitudinally based on the albumin tertiles at baseline, using binary Cox proportional hazard analysis. When analyzing the OR for the presence of NAFLD, subjects with alcohol intake >20 g/day were excluded.
RESULTS
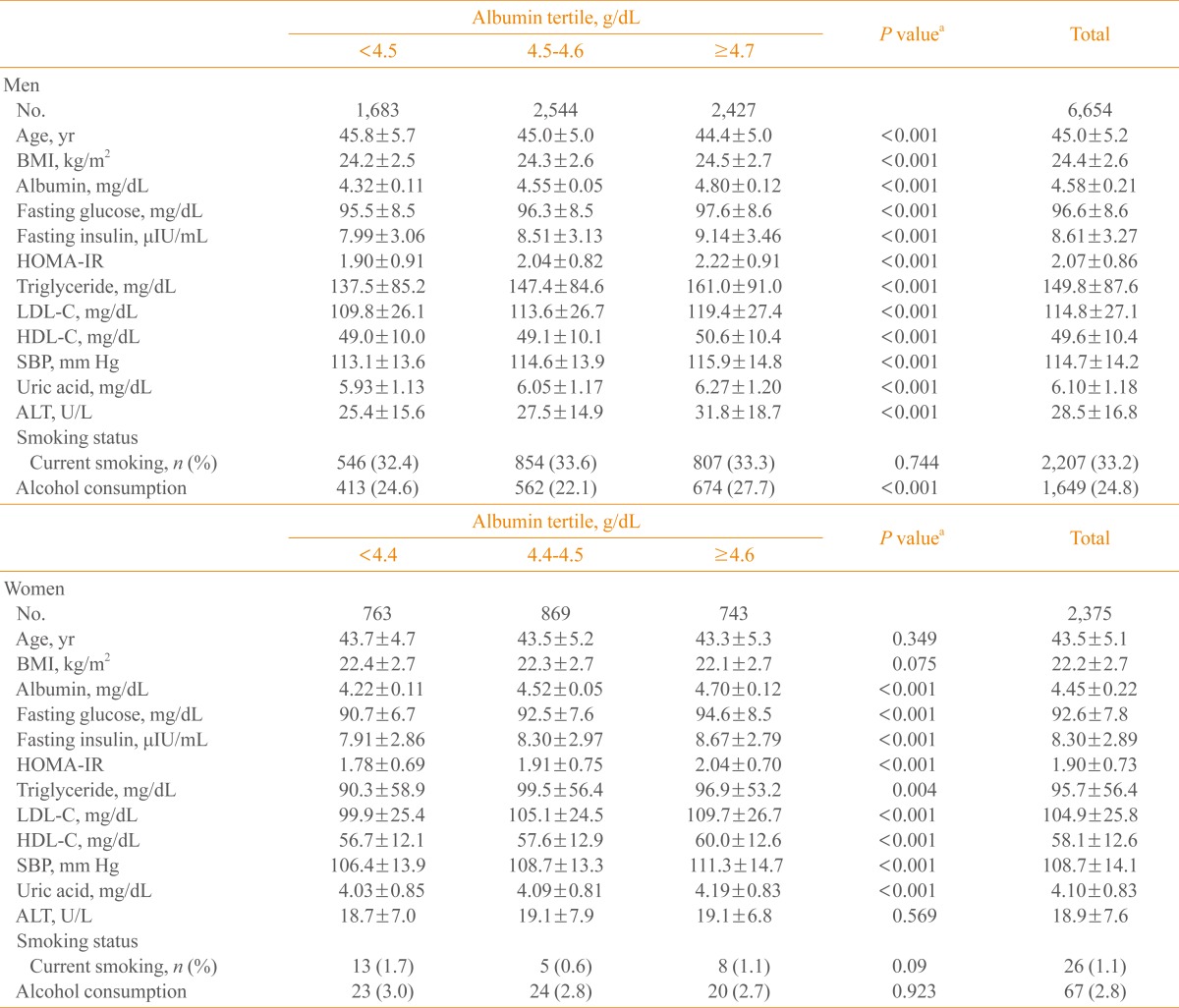
Table 1 shows the baseline characteristics of the study subjects by tertiles of serum albumin. Fasting glucose, fating insulin, HOMA-IR, systolic BP, uric acid, and low density lipoprotein cholesterol increased with increasing albumin tertiles, in both men and women.
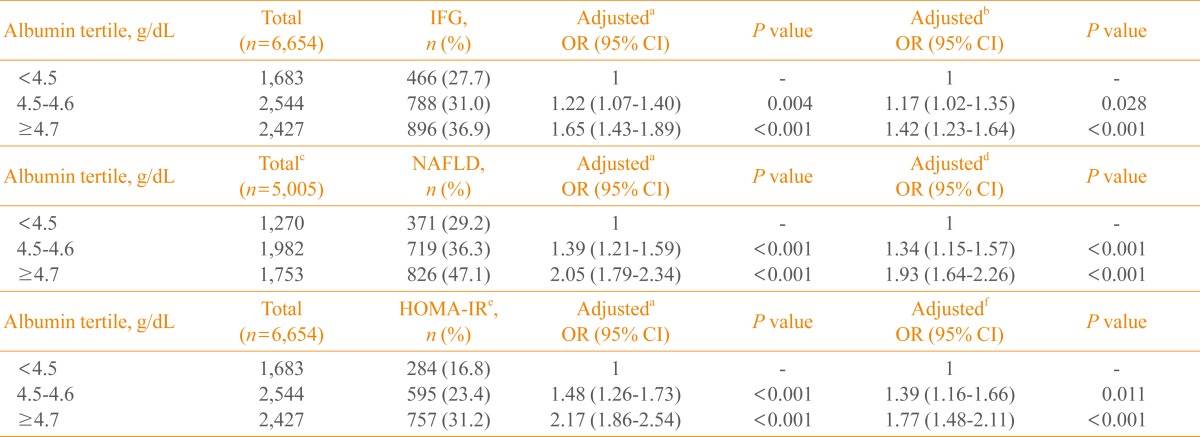
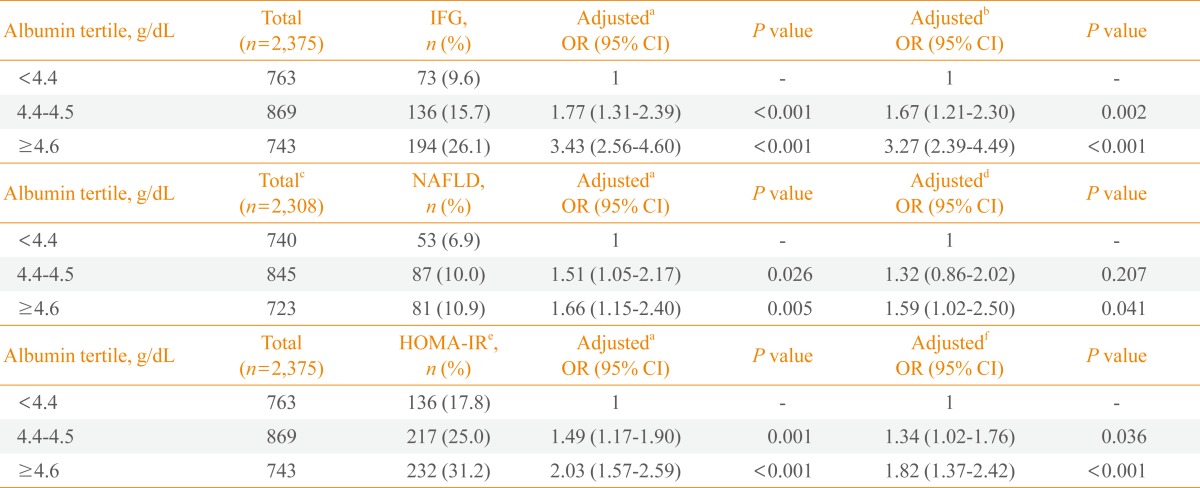
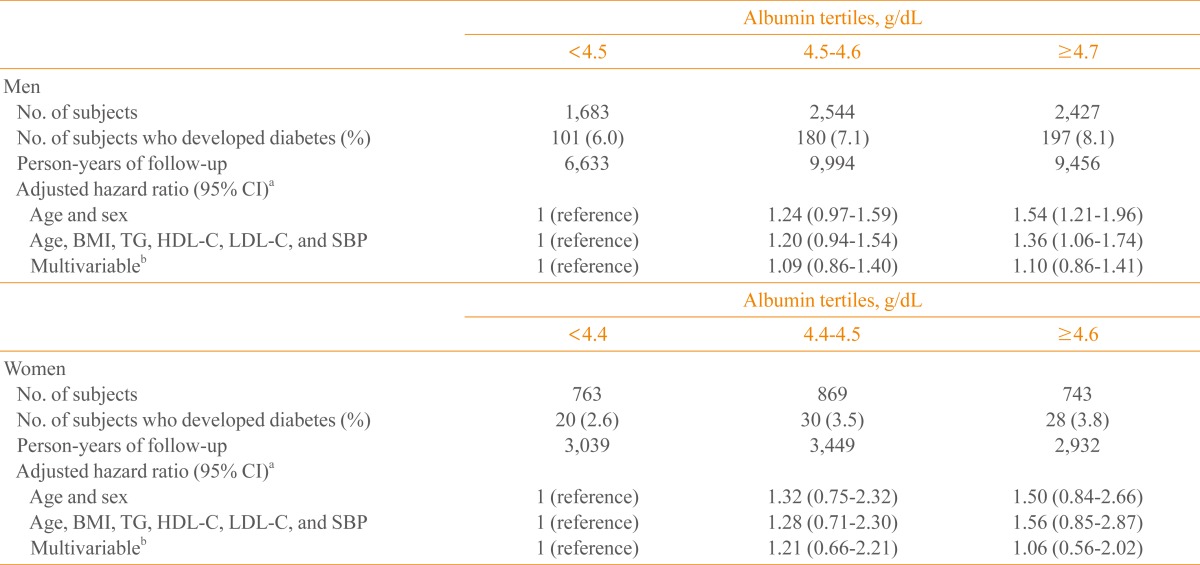
From the lowest to the highest tertile of albumin, the multivariable-adjusted ORs of insulin resistance (defined as the top quartile of HOMA-IR and the presence of IFG and NAFLD) increased significantly in both men and women (Tables 2, 3). During the mean follow-up period of nearly 4 years (47.2 months), 556 (6.1%, 478 men and 78 women) of the 9,029 subjects progressed to diabetes. In the Cox proportional hazard model, after adjusting for age, body mass index, triglyceride, high density lipoprotein cholesterol, systolic BP, presence of IFG and fatty liver, smoking status, and alcohol consumption, the HRs (95% confidence interval [CI]) of diabetes in men were 1, 1.09 (95% CI, 0.86 to 1.40), and 1.10 (95% CI, 0.86 to 1.41), respectively, from the lowest to the highest tertile of albumin. Corresponding values for women were 1, 1.21 (95% CI, 0.66 to 2.21), and 1.06 (95% CI, 0.56 to 2.02), respectively (Table 4).
DISCUSSION
In our study, serum albumin concentration was associated with higher levels of HOMA-IR, and the presence of IFG and NAFLD in nondiabetic subjects. Several studies have also reported that serum albumin was positively associated with metabolic syndrome or metabolic risk factors including lipid profile, BP, and body mass index [6,17-19]. These results suggest that serum albumin is associated with insulin resistance.
Insulin resistance is a principal cause of type 2 diabetes [20] and serum albumin has been associated with insulin resistance [6,17-19]. However, in our study, serum albumin did not have independent effect on the development of diabetes. Although it is not clear whether there is causal relationship between insulin resistance and serum albumin levels, our results indicate that insulin resistance may affect serum albumin levels. Insulin resistance is by definition linked to hyperinsulinemia [21]. Nondiabetic patients with insulin resistance have compensatory hyperinsulinemia, a state which predisposes to the development of metabolic impairments, including nonalcoholic fatty liver disease, IFG, and metabolic syndrome [14,22]. This compensatory hyperinsulinemia may contribute to this relationship between insulin resistance and serum albumin levels. Several studies investigating the possibility of a direct relationship between insulin and albumin synthesis have provided insight into that theory. Insulin has effects on the synthesis rates of liver proteins such as albumin and fibrinogen. In vivo in rats and in rat hepatocytes cultures, insulin increased albumin gene transcription and mRNA synthesis in a dose-dependent manner [23,24]. In contrast, insulin deficiency decreased both albumin gene transcription and mRNA concentration with a resultant decrease of albumin synthesis [23-25]. Additionally, in type 1 diabetes patients, insulin withdrawal resulted in a decrease in the albumin synthetic rate, with these changes being reversed by insulin [26]. In diabetic patients, however, plasma albumin concentration has been reported to be inversely related with HbA1c levels, revealing a large proportion of poorly controlled diabetes in patients with lower plasma albumin concentrations [27]. This inverse relationship may also be explained by the fact that poorly controlled type 2 diabetes has been associated with a further decrease in insulin production and secretion by the pancreatic β-cell [28,29].
While our results and those previously reported in other studies show that increased serum albumin is associated with several atherogenic risk factors including lipid profile, BP, body mass index, and insulin resistance [6], several prospective studies have demonstrated the cardioprotective role of serum albumin as lower concentrations of serum albumin were associated with increased risk of coronary heart disease, cardiovascular mortality and carotid atherosclerosis [7,30]. The antioxidant and anti-inflammatory properties of serum albumin in the atherogenetic process have been suggested as possible mechanisms for this inverse association [6-10]. Oxidative stress and chronic inflammation play crucial roles in the generation of both insulin resistance and type 2 diabetes [11,12]. The reported antioxidant and anti-inflammatory properties of serum albumin indicate that serum albumin may have an independent protective effect on incident diabetes, as observed in the association with carotid atherosclerosis and cardiovascular mortality. However, in our study, serum albumin did not have a protective effect on incident diabetes, suggesting that serum albumin does not have anti-inflammatory or antioxidant properties in the development of diabetes.
A limitation in the current study was that we did not use the 2 hours postload glucose test for diagnosing diabetes. This may have included subjects with undiagnosed diabetes at baseline and underestimated the development of diabetes during the follow-up period. Likewise, the self-reporting of diabetes and use of diabetic medications on the questionnaires included in our assessment of diabetes development may have also led to under-reporting of diabetes. Finally, the use of ultrasonography to diagnose NAFLD was another limitation in our study. Although our ultrasonography exams were performed by several experienced radiologists, we did not assess interobserver reliability or consider the degree of fatty liver.
In conclusion, our study showed that increased serum albumin level is associated with insulin resistance. However, analysis of the causal relationship indicated that serum albumin did not have an independent effect on the development of diabetes.
 XML Download
XML Download