

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Struma ovarii is a rare monodermal variant of ovarian teratoma accounting for only 2% of all mature teratomas. To be classified as a struma ovarii, teratoma must be composed predominantly of mature thyroid tissue (> 50%). This tumor is generally benign, although malignant transformation has been reported. Struma ovarii occur mostly as unilateral cases, so bilateral cases are quite rare (less than 6% of cases). Struma ovarii occur largely without symptoms or are accompanied by non-specific symptoms, such as abdominal pain, a palpable abdominal mass, and abdominal distension. The preoperative diagnosis is generally difficult. The incidence of hyperthyroidism has been reported to be 5-10% of patients with struma ovarii. Thus, cases of functional bilateral struma ovarii are very rare. We report a case of bilateral struma ovarii with subclinical thyrotoxicosis and a diffuse goiter, mimicking a malignant ovarian tumor, and include a brief review of related literature.
Figures and Tables
Fig. 1
T1WI magnetic resonance imaging with gadolinium enhancement shows bilateral ovarian masses. A. Right ovarian mass measuring 11 × 9 cm in its largest diameter with multiple septated cystic and solid portion is noted. B. Left ovarian mass measuring 7 × 4.5 cm in its largest diameter with suspicious enhancing solid portion is also noted.
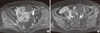
Fig. 2
Thyroid utrasonography shows relatively well defined hypoechoic nodule in right thyroid gland (A) and isoechoic nodules in left thyroid gland (B) with moderate
diffuse goiter.
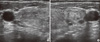
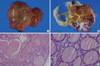
Fig. 4
A. Right ovary shows multiple cysts and smooth surface in gross finding. B. Cut surface of right ovary shows compartment of ambor-colored thyroid tissue separated by thick fibrous septae in gross finding. C, D. Thyroid tissues with colloid filled follicles varying in size, lined by flat to cuboidal cells with representing struma ovarii are noted in microscopic findings (C, H&E stain, × 40; D, H&E stain, × 400).
References
1. Dardik RB, Dardik M, Westra W, Montz FJ. Malignant struma ovarii: two case reports and a review of the literature. Gynecol Oncol. 1999. 73:447–451.
2. Gould SF, Lopez RL, Speers WC. Malignant struma ovarii. A case report and literature review. J Reprod Med. 1983. 28:415–419.
3. Fleuren GJ, Coerkamp EG, Nap M, vd Broek LJ, Warnaar SO. Immunohistological characterization of a monoclonal antibody (OV632) against epithelial ovarian carcinomas. Virchows Arch A Pathol Anat Histopathol. 1987. 410:481–486.
4. Woodruff JD, Rauh JT, Markley RL. Ovarian struma. Obstet Gynecol. 1966. 27:194–201.
5. Hasleton PS, Kelehan P, Whittaker JS, Burslem RW, Turner L. Benign and malignant struma ovarii. Arch Pathol Lab Med. 1978. 102:180–184.
6. Pardo-Mindan FJ, Vazquez JJ. Malignant struma ovarii. Light and electron microscopic study. Cancer. 1983. 51:337–343.
7. Ayhan A, Yanik F, Tuncer R, Tuncer ZS, Ruacan S. Struma ovarii. Int J Gynaecol Obstet. 1993. 42:143–146.
8. Smith FC. Pathology and physiology of struma ovarii. Arch Surg. 1946. 53:603–626.
9. Grandet PJ, Remi MH. Struma ovarii with hyperthyroidism. Clin Nucl Med. 2000. 25:763–765.
10. Kim SJ, Pak K, Lim HJ, Yun KH, Seong SJ, Kim TJ, Lim KT, Jung HW, Park IS, Shim JU, Park CT, Lee KH. Clinical diversity of struma ovarii. Korean J Obstet Gynecol. 2002. 45:748–752.
11. Kempers RD, Dockerty MB, Hoffman DL, Bartholomew LG. Struma ovarii: ascitic, hyperthyroid, and asymptomatic syndromes. Ann Intern Med. 1970. 72:883–893.
12. Devaney K, Snyder R, Norris HJ, Tavassoli FA. Proliferative and histologically malignant struma ovarii: a clinicopathologic study of 54 cases. Int J Gynecol Pathol. 1993. 12:333–343.
13. Rosenblum NG, LiVolsi VA, Edmonds PR, Mikuta JJ. Malignant struma ovarii. Gynecol Oncol. 1989. 32:224–227.
14. O'Connell ME, Fisher C, Harmer CL. Malignant struma ovarii: presentation and management. Br J Radiol. 1990. 63:360–363.
15. Berghella V, Ngadiman S, Rosenberg H, Hoda S, Zuna RE. Malignant struma ovarii. A case report and review of the literature. Gynecol Obstet Invest. 1997. 43:68–72.
16. Ronga G, Fiorentino A, Paserio E, Signore A, Todino V, Tummarello MA, Filesi M, Baschieri I. Can iodine-131 whole-body scan be replaced by thyroglobulin measurement in the post-surgical follow-up of differentiated thyroid carcinoma? J Nucl Med. 1990. 31:1766–1771.
17. Lubin E, Mechlis-Frish S, Zatz S, Shimoni A, Segal K, Avraham A, Levy R, Feinmesser R. Serum thyroglobulin and iodine-131 whole-body scan in the diagnosis and assessment of treatment for metastatic differentiated thyroid carcinoma. J Nucl Med. 1994. 35:257–262.
 XML Download
XML Download