

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Ectopic thyroid glands generally occur in the midline as a result of abnormal median migration and their presence in lateral to the midline is rare. Embryologically, the thyroid gland is derived from two anlages: a large median endodermal anlage and two lateral anlages. The median anlage produces most of the thyroid parenchyma, whereas the lateral anlage is derived from the fourth pharyngeal pouch and contributes 1-30% of the thyroid weight. In rare cases, failure of the lateral anlage to fuse with the median anlage can result in lateral ectopic thyroid gland. For many years, lateral, aberrant thyroid tissue in adults was a term used almost exclusively for metastatic thyroid carcinoma. However, aberrant, benign ectopic thyroid tissue rarely occurs. We present a 47-year-old man who had incidentally detected mass on the right lateral neck. He was clinically in a euthyroid status and the thyroid function test results were normal as well. Neck ultrasonography revealed a mild diffuse goiter and a 1.22 × 0.65 cm sized ovoid mass like lesion was located in the right level IV of the neck. The result of fine needle aspiration cytology was adenomatous goiter without lymphoid tissue or any malignancy. We rarely report aberrant, benign ectopic thyroid presence as a lateral neck mass.
Figures and Tables
Fig. 1
Technetium-99m (99mTc) thyroid scan. 99mTc thyroid scan shows mild diffuse enlargement of the thyroid gland. Lateral neck mass was invisible on thyroid scan.

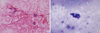
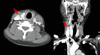
Fig. 2
Ultrasonography of thyroid gland. Ultrasonography of thyroid gland shows a 1.22 × 0.65 cm sized ovoid mass like lesion in right level IV (white arrow). (A) Transverse view. (B) Longitudinal view. (C) Color Doppler image shows a mass with peripheral vascularity. (D) Follow-up ultrasonography image shows no significant interval change.

References
1. Baik SH, Choi JH, Lee HM. Dual ectopic thyroid. Eur Arch Otorhinolaryngol. 2002. 259:105–107.
2. Hazarika P, Siddiqui SA, Pujary K, Shah P, Nayak DR, Balakrishnan R. Dual ectopic thyroid: a report of two cases. J Laryngol Otol. 1998. 112:393–395.
3. Macchia PE, Lapi P, Chiovato L, Busslinger M, Fenzi GF, DiLauro R. Identification of a mutation in the PAX-8 gene in a patient with thyroid ectopy. J Endocrinol Invest. 1997. 20:Suppl 5. 84.
4. Abramowicz MJ, Vassart G, Refetoff S. Probing the cause of thyroid dysgenesis. Thyroid. 1997. 7:325–326.
5. Macchia PE, Lapi P, Krude H, Pirro MT, Missero C, Chiovato L, Souabni A, Baserga M, Tassi V, Pinchera A, Fenzi G, Gruters A, Busslinger M, Di Lauro R. PAX8 mutations associated with congenital hypothyroidism caused by thyroid dysgenesis. Nat Genet. 1998. 19:83–86.
6. Congdon T, Nguyen LQ, Nogueira CR, Habiby RL, Medeiros-Neto G, Kopp P. A novel mutation (Q40P) in PAX8 associated with congenital hypothyroidism and thyroid hypoplasia: evidence for phenotypic variability in mother and child. J Clin Endocrinol Metab. 2001. 86:3962–3967.
7. Alt B, Elsalini OA, Schrumpf P, Haufs N, Lawson ND, Schwabe GC, Mundlos S, Gruters A, Krude H, Rohr KB. Arteries define the position of the thyroid gland during its developmental relocalisation. Development. 2006. 133:3797–3804.
8. Yoon JS, Won KC, Cho IH, Lee JT, Lee HW. Clinical characteristics of ectopic thyroid in Korea. Thyroid. 2007. 17:1117–1121.
9. Duong RB, Fernandez-Ulloa M, Planitz MK, Maxon HR. I-123 breast uptake in a young primipara with postpartum transient thyrotoxicosis. Clin Nucl Med. 1983. 8:35.
10. Kumar R, Gupta R, Bal CS, Khullar S, Malhotra A. Thyrotoxicosis in a patient with submandibular thyroid. Thyroid. 2000. 10:363–365.
11. Hari CK, Brown MJ, Thompson I. Tall cell variant of papillary carcinoma arising from ectopic thyroid tissue in the trachea. J Laryngol Otol. 1999. 113:183–185.
12. Sand J, Pehkonen E, Mattila J, Seppănen S, Salmi J. Pulsating mass at the sternum: a primary carcinoma of ectopic mediastinal thyroid. J Thorac Cardiovasc Surg. 1996. 112:833–835.
13. Massine RE, Durning SJ, Koroscil TM. Lingual thyroid carcinoma: a case report and review of the literature. Thyroid. 2001. 11:1191–1196.
14. Hod N, Mindlin L, Cohenpour M, Horne T. Double ectopic thyroid. Pediatr Radiol. 2002. 32:859–861.
15. Kim DY, Yang SH, Song SH, Park JS. Dual ectopic thyroid. Korean J Otolaryngol-Head Neck Surg. 2001. 44:1120–1122.
16. Kalan A, Tariq M. Lingual thyroid gland: clinical evaluation and comprehensive management. Ear Nose Throat J. 345. 78:340–341. 345–349.
17. Williams JD, Sclafani AP, Slupchinskij O, Douge C. Evaluation and management of the lingual thyroid gland. Ann Otol Rhinol Laryngol. 1996. 105:312–316.
 XML Download
XML Download