

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Background
Thyroid function depends on ethnic and environmental factors. North Korean refugees have the same genetic background as South Koreans, but they have been exposed to different environments. This study examines the prevalence and pattern of thyroid disorders in North Korean women living in South Korea, focusing on subclinical hypothyroidism (SCH).
Methods
The intended sample was a total of 327 North Korean women residing in Seoul. Health questionnaires and medical examinations, including serum thyrotropin (thyroid stimulating hormone, TSH), free thyroxine, and thyroid autoantibodies, were conducted.
Results
The prevalence of SCH was 9.4%. In logistic regression analysis, smoking, menopause, length of stay in South Korea, body mass index, history of thyroid disease, and metabolic syndrome were not associated with the risk of SCH. Whereas, the positivity of autoantibodies were associated with a high risk for SCH (odds ratio [OR], 4.840; 95% confidence interval [CI], 1.80-13.017; P = 0.002), and age was associated with a low risk for SCH (OR, 0.94; 95% CI, 0.888-0.994; P = 0.031). The serum TSH levels also decreased with increasing age, and in particular, there was significant difference between 30-39 years, and over 60 years (2.33 ± 1.51 µIU/mL vs. 1.54 ± 0.73 µIU/mL, P = 0.028).
Conclusion
In North Korean women, the positivity of autoantibodies was associated with a high risk for SCH. But interestingly, a younger age was associated with a high risk for SCH. Considering that they suffered from severe famine at the period of growth, and this led to malnutrition, their thyroid dysfunction might be associated with the peculiar environment that they experienced.
Figures and Tables
Fig. 1
Prevalence of subclinical hypothyroidism (SCH) and positivity of autoantibody according to age groups. The younger they are, the more prevalence of SCH was increased (P for trend = 0.011). But such trend was not seen in presence of autoantibody.

Fig. 2
Comparison of free T4 and thyroid stimulating hormone concentration according to age groups. The differences between groups were evaluated using one-way ANOVA with Bonferroni's post hoc test (thyroid stimulating hormone [TSH], 30-39 vs. 60-, 2.33 ± 1.51 vs. 1.54 ± 0.73, P = 0.028; free thyroxine [free T4], 30-39 vs. 40-49, 1.35 ± 0.18 vs. 1.28 ± 0.16, P = 0.021).
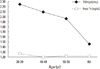


Table 3
Comparison of characteristics between euthyroid and subclinical hypothyroid subjects

Values are expressed as median, mean ± SD or percentage (n).
CES-D, Center for Epidemiological Studies-Depression Scale; Free T4, free thyroxine; HDL-C, high density lipoprotein cholesterol; HOMA-IR, homeostatic model assessment for insulin resistance; LDL-C, low density lipoprotein cholesterol; PWI-SF, Psychosocial Well-Being Index-Short Form; SCH, subclinical hypothyroidism; TSH, thyroid stimulating hormone.

References
1. Cho BY. The clinical thyroidology. 2010. 3rd ed. Seoul: Korea Medical Book.
2. Hollowell JG, Staehling NW, Flanders WD, Hannon WH, Gunter EW, Spencer CA, Braverman LE. Serum TSH, T(4), and thyroid antibodies in the United States population (1988 to 1994): National Health and Nutrition Examination Survey (NHANES III). J Clin Endocrinol Metab. 2002. 87:489–499.
3. Chung JH, Kim BJ, Choi YH, Shin MH, Kim SH, Min YK, Lee MS, Lee MG, Kim KW. Prevalence of thyrotoxicosis and hypothyroidism in the subjects for health check-up. J Korean Soc Endocrinol. 1999. 14:301–313.
4. Oh MK, Cheon KS, Jung SM, Ryu DS, Park MS, Cheong SS, Kim JS, Park BG. Prevalence of thyroid diseases among adult for health check-up in a Youngdong area of Kwangwon province. J Korean Acad Fam Med. 2001. 22:1363–1374.
5. Jang HW, Lee JI, Shin HW, Kim SW, Min YK, Lee MS, Lee MK, Kim KW, Chung JH. Reference range of serum TSH with aging and prevalence of subclinical hypothyroidism in patients without history of thyroid disease for the general medical examination. J Korean Thyroid Assoc. 2009. 2:28–32.
6. Choi HS, Park YJ, Kim HK, Choi SH, Lim S, Park DJ, Jang HC, Cho NH, Cho BY. Prevalence of subclinical hypothyroidism in two population based-Cohort: Ansung and KLoSHA Cohort in Korea. J Korean Thyroid Assoc. 2010. 3:32–40.
7. Kim WB. Recent progress in research on autoimmune thyroid diseases. J Korean Soc Endocrinol. 2002. 17:338–357.
8. Lantz M, Abraham-Nordling M, Svensson J, Wallin G, Hallengren B. Immigration and the incidence of Graves' thyrotoxicosis, thyrotoxic multinodular goiter and solitary toxic adenoma. Eur J Endocrinol. 2009. 160:201–206.
9. Moradi T, Nordqvist T, Allebeck P, Galanti MR. Risk of thyroid cancer among Iranian immigrants in Sweden. Cancer Causes Control. 2008. 19:221–226.
10. Lee YH, Lee WJ, Kim YJ, Cho MJ, Kim JH, Lee YJ, Kim HY, Choi DS, Kim SG, Robinson C. North Korean refugee health in South Korea (NORNS) study: study design and methods. BMC Public Health. 2012. 12:172.
11. Lee MS. Epidemiologic studies-depression scale in the Korean version. Health Soc Sci. 2002. 12:43–62.
12. Lee CY, Lee JY. Reliability and validity of PWI (psychosocial wellbeing index). Korean J Prev Med. 1996. 29:255–264.
13. Haggard S, Noland M. Reform from below: behavioral and institutional change in North Korea. J Econ Behav Organ. 2010. 73:133–152.
14. Ministry of Unification. Current status of north Korean refugees' resettlement [Internet]. 2011. cited 2012 April 20. Seoul: Ministry of Unification;Available from: http://www.unikorea.go.kr/CmsWeb/viewPage.req?idx=PG0000000365.
15. Salvatore D, Davies TF, Schlumberger MJ, Hay ID, Larsen PR. Melmed S, Polonsky KS, Larson PR, Kronenberg HM, editors. Thyroid physiology and diagnostic evaluation of patients with thyroid disorders. Williams Textbook of Endocrinology. 2011. 12th ed. Philadelphia: Elsevier/Saunders;327–361.
16. Guo J, Wang Y, Rapoport B, McLachlan SM. Evidence for antigen presentation to sensitized T cells by thyroid peroxidase (TPO)-specific B cells in mice injected with fibroblasts co-expressing TPO and MHC class II. Clin Exp Immunol. 2000. 119:38–46.
17. Mariotti S, Caturegli P, Piccolo P, Barbesino G, Pinchera A. Antithyroid peroxidase autoantibodies in thyroid diseases. J Clin Endocrinol Metab. 1990. 71:661–669.
18. Chu JW, Crapo LM. The treatment of subclinical hypothyroidism is seldom necessary. J Clin Endocrinol Metab. 2001. 86:4591–4599.
19. Holm IA, Manson JE, Michels KB, Alexander EK, Willett WC, Utiger RD. Smoking and other lifestyle factors and the risk of Graves' hyperthyroidism. Arch Intern Med. 2005. 165:1606–1611.
20. Prummel MF, Wiersinga WM. Smoking and risk of Graves' disease. JAMA. 1993. 269:479–482.
21. Vestergaard P. Smoking and thyroid disorders: a meta-analysis. Eur J Endocrinol. 2002. 146:153–161.
22. Vestergaard P, Rejnmark L, Weeke J, Hoeck HC, Nielsen HK, Rungby J, Laurberg P, Mosekilde L. Smoking as a risk factor for Graves' disease, toxic nodular goiter, and autoimmune hypothyroidism. Thyroid. 2002. 12:69–75.
23. Belin RM, Astor BC, Powe NR, Ladenson PW. Smoke exposure is associated with a lower prevalence of serum thyroid autoantibodies and thyrotropin concentration elevation and a higher prevalence of mild thyrotropin concentration suppression in the third National Health and Nutrition Examination Survey (NHANES III). J Clin Endocrinol Metab. 2004. 89:6077–6086.
24. Kim BH, Kim WB, Kim TY, Kim HK, Jeon SH, Lee CW, Shong YK. Association between cigarette smoking and thyroid function in adults without previous history of thyroid disease. J Korean Endocr Soc. 2008. 23:123–128.
25. Cho NH, Choi HS, Kim KW, Kim HL, Lee SY, Choi SH, Lim S, Park YJ, Park do J, Jang HC, Cho BY. Interaction between cigarette smoking and iodine intake and their impact on thyroid function. Clin Endocrinol (Oxf). 2010. 73:264–270.
26. Chiovato L, Pinchera A. Stressful life events and Graves' disease. Eur J Endocrinol. 1996. 134:680–682.
27. Pop VJ, Maartens LH, Leusink G, van Son MJ, Knottnerus AA, Ward AM, Metcalfe R, Weetman AP. Are autoimmune thyroid dysfunction and depression related? J Clin Endocrinol Metab. 1998. 83:3194–3197.
28. Strieder TG, Prummel MF, Tijssen JG, Brosschot JF, Wiersinga WM. Stress is not associated with thyroid peroxidase autoantibodies in euthyroid women. Brain Behav Immun. 2005. 19:203–206.
29. Surks MI, Hollowell JG. Age-specific distribution of serum thyrotropin and antithyroid antibodies in the US population: implications for the prevalence of subclinical hypothyroidism. J Clin Endocrinol Metab. 2007. 92:4575–4582.
30. Kajantie E, Phillips DI, Osmond C, Barker DJ, Forsén T, Eriksson JG. Spontaneous hypothyroidism in adult women is predicted by small body size at birth and during childhood. J Clin Endocrinol Metab. 2006. 91:4953–4956.
31. Kivity S, Agmon-Levin N, Zisappl M, Shapira Y, Nagy EV, Danko K, Szekanecz Z, Langevitz P, Shoenfeld Y. Vitamin D and autoimmune thyroid diseases. Cell Mol Immunol. 2011. 8:243–247.
32. UNICEF. Sustainable elimination of iodine deficiency [Internet]. 2008. cited 2012 April 20. New York: UNICEF;Available from: http://www.unicef.org/media/files/IDD.pdf.
 XML Download
XML Download