

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
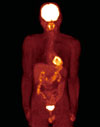
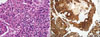
Intra-operative parathyroid hormone (IOPTH) assay is a useful tool to confirm complete excision of all hyper-functioning parathyroid gland tissue. In this report, we describe a case with successful localization of distant metastasis in a patient with parathyroid carcinoma using the IOPTH assay. A 53-year-old man presented to our clinic with a serum calcium level of 11.8 mg/dL and an intact PTH level of 233.3 pg/mL. He had been treated for parathyroid carcinoma eleven years ago. Two suspected metastatic lesions were detected on the chest computed tomography. Due to the vastly different surgical field necessary to excise each lesion, we preferentially removed only one lesion and we monitored the other remaining suspected lesion without resection via IOPTH assay. Six months later, the patient's serum calcium and intact PTH levels remained within their normal ranges. To the best of our knowledge, this is the first case to effectively utilize IOPTH assay for the management of metastatic parathyroid carcinoma.
Figures and Tables
Fig. 1
Intraoperative parathyroid hormone (PTH) level remained high even after removal of the two remaining parathyroid glands (A). Intraoperative parathyroid hormone fell to < 50% of baseline within five minutes after the resection of right pulmonary nodule (B).


References
1. Busaidy NL, Jimenez C, Habra MA, Schultz PN, El-Naggar AK, Clayman GL, Asper JA, Diaz EM Jr, Evans DB, Gagel RF, Garden A, Hoff AO, Lee JE, Morrison WH, Rosenthal DI, Sherman SI, Sturgis EM, Waguespack SG, Weber RS, Wirfel K, Vassilopoulou-Sellin R. Parathyroid carcinoma: a 22-year experience. Head Neck. 2004. 26:716–726.
2. Rodgers SE, Perrier ND. Parathyroid carcinoma. Curr Opin Oncol. 2006. 18:16–22.
3. Givi B, Shah JP. Parathyroid Carcinoma. Clin Oncol (R Coll Radiol). 2010. 22:498–507.
4. Lee JH, Kim YM, Hwang DS, Hwang YT, Eum JB, Seo JM, Choi DH, Kang BS, Noh YJ, Nam-Goong IS, Kim YI, Kim ES. A case of parathyroid carcinoma underwent radiation therapy on the metastatic bone lesions. J Korean Endocr Soc. 2007. 22:344–352.
5. Lee YS, Hong SW, Jeong JJ, Nam KH, Chung WY, Chang HS, Park CS. Parathyroid carcinoma: a 16-year experience in a single institution. Endocr J. 2010. 57:493–497.
6. Kebebew E. Parathyroid carcinoma. Curr Treat Options Oncol. 2001. 2:347–354.
7. Shane E. Clinical review 122: Parathyroid carcinoma. J Clin Endocrinol Metab. 2001. 86:485–493.
8. Kebebew E, Arici C, Duh QY, Clark OH. Localization and reoperation results for persistent and recurrent parathyroid carcinoma. Arch Surg. 2001. 136:878–885.
9. Obara T, Okamoto T, Ito Y, Yamashita T, Kawano M, Nishi T, Tani M, Sato K, Demura H, Fujimoto Y. Surgical and medical management of patients with pulmonary metastasis from parathyroid carcinoma. Surgery. 1993. 114:1040–1049.
10. Koea JB, Shaw JH. Parathyroid cancer: biology and management. Surg Oncol. 1999. 8:155–165.
11. Kebebew E, Clark OH. Parathyroid adenoma, hyperplasia, and carcinoma: localization, technical details of primary neck exploration, and treatment of hypercalcemic crisis. Surg Oncol Clin N Am. 1998. 7:721–748.
12. Hessman O, Stalberg P, Sundin A, Garske U, Rudberg C, Eriksson LG, Hellman P, Akerstrom G. High success rate of parathyroid reoperation may be achieved with improved localization diagnosis. World J Surg. 2008. 32:774–783.
13. Neumann DR, Esselstyn CB, MacIntyre WJ, Chen EQ, Go RT, Kohse LM. Parathyroid adenoma localization by PET FDG. J Comput Assist Tomogr. 1993. 17:976–977.
14. Melon P, Luxen A, Hamoir E, Meurisse M. Fluorine-18-fluorodeoxyglucose positron emission tomography for preoperative parathyroid imaging in primary hyperparathyroidism. Eur J Nucl Med. 1995. 22:556–558.
15. Neumann DR, Esselstyn CB, Siciliano D, MacIntyre WJ, Kohse LM, Licata AA. Preoperative imaging of parathyroid carcinoma by positron emission tomography. Ann Otol Rhinol Laryngol. 1994. 103:741–745.
16. Irvin GL 3rd, Dembrow VD, Prudhomme DL. Clinical usefulness of an intraoperative "quick parathyroid hormone" assay. Surgery. 1993. 114:1019–1023.
17. Habener JF, Rosenblatt M, Potts JT Jr. Parathyroid hormone: biochemical aspects of biosynthesis, secretion, action, and metabolism. Physiol Rev. 1984. 64:985–1053.
18. Irvin GL 3rd, Molinari AS, Figueroa C, Carneiro DM. Improved success rate in reoperative parathyroidectomy with intraoperative PTH assay. Ann Surg. 1999. 229:874–879.
19. Barczynski M, Konturek A, Cichon S, Hubalewska-Dydejczyk A, Golkowski F, Huszno B. Intraoperative parathyroid hormone assay improves outcomes of minimally invasive parathyroidectomy mainly in patients with a presumed solitary parathyroid adenoma and missing concordance of preoperative imaging. Clin Endocrinol (Oxf). 2007. 66:878–885.
20. Hundahl SA, Fleming ID, Fremgen AM, Menck HR. The American College of Surgeons Commission on Cancer and the American Cancer Society. Two hundred eighty-six cases of parathyroid carcinoma treated in the U.S. between 1985-1995: a National Cancer Data Base Report. Cancer. 1999. 86:538–544.
 XML Download
XML Download