

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Background
Various staging systems for thyroid cancer that focus on cancer specific death have been suggested, but this approach had a limitation due to the relatively long clinical course and very low rate of cancer death. This study was performed to evaluate the staging systems and to determine the most predictive staging system for predicting recurrence.
Methods
The patients who underwent first total or near total thyroidectomy due to papillary thyroid cancer (PTC) at Asan Medical Center between January 1995 and December 2001 were the subjects of this study. The commonly used 8 staging systems were applied to these subjects. Disease free survival (DFS) and the relative importance of each staging system were determined by the Kaplan-Meier method, the Cox-proportional hazards model and the proportion of variation in the survival time explained (PVE).
Results
A total of 952 patients (M = 117, F = 835) were enrolled and their mean age was 45 years. During a median of 10 years of follow-up, 146 (15.3%) of 952 patients had recurred tumor. The independent prognostic factors were male gender, tumor size, extrathyroidal invasion and cervical lymph node metastasis. Risk stratification according to the American thyroid association (ATA) guideline was the most predictive staging system for recurrence of PTC (PVE 88.6%). The staging systems from EORTC (PVE 79.5%), and MACIS (PVE 68.4%) had significant values for predicting recurrence of PTC. The stage of NTCTCS could not predict recurrence (PVE 4.5%, P = 0.11).
Figures and Tables
Fig. 1
Disease-free survival of papillary thyroid carcinoma according to EORTC staging system (A), AMES (B), Clinical class (C), and MACIS (D). EORTC, staging of European Organization for Research and Treatment of Cancer; AMES, age, metastasis, extent and size; MACIS, metastasis, age, completeness of resection, invasion and size.

Fig. 2
Disease-free survival of papillary thyroid carcinoma according to staging of OSU (A), NTCTCS (B), AJCC/UICC TNM staging (C), and risk stratification of ATA guideline (D). OSU, staging of Ohio State University; NTCTCS, staging of National Thyroid Cancer Treatment Cooperative Study; AJCC, American Joint Committee on Cancer; UICC, International Union against Cancer; TNM, tumor, lymph nodes, and metastasis; ATA, American Thyroid Association.


Table 2
Clinicopatholgoical parameters associated with clinical recurrence of papillary thyroid carcinoma

Table 3
Proportion of variation explained and ranking of the various staging systems for papillary thyroid carcinoma
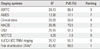
G2, maximum likelihood ratio; PVE, proportion of variation in survival time explained; EORTC, staging of European Organization for Research and Treatment of Cancer; AMES, age, metastasis, extent and size; MACIS, metastasis, age, completeness of resection, invasion and size; OSU, staging of Ohio State University; NTCTCS, staging of National Thyroid Cancer Treatment Cooperative Study; AJCC, American Joint Committee on Cancer; UICC, International Union against Cancer; TNM, tumor, lymph nodes, and metastasis; ATA, American Thyroid Association.
*Risk stratification for recurrence of thyroid cancer according to ATA guideline.
References
1. Cooper DS, Doherty GM, Haugen BR, Kloos RT, Lee SL, Mandel SJ, Mazzaferri EL, McIver B, Sherman SI, Tuttle RM. Management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2006. 16:109–142.
2. Pacini F, Schlumberger M, Dralle H, Elisei R, Smit JW, Wiersinga W. European consensus for the management of patients with differentiated thyroid carcinoma of the follicular epithelium. Eur J Endocrinol. 2006. 154:787–803.
3. Cooper DS, Doherty GM, Haugen BR, Kloos RT, Lee SL, Mandel SJ, Mazzaferri EL, McIver B, Pacini F, Schlumberger M, Sherman SI, Steward DL, Tuttle RM. Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2009. 19:1167–1214.
4. Byar DP, Green SB, Dor P, Williams ED, Colon J, van Gilse HA, Mayer M, Sylvester RJ, van Glabbeke M. Thyroid Cancer Cooperative Group. A prognostic index for thyroid carcinoma. A study of the E.O.R.T.C. Eur J Cancer. 1979. 15:1033–1041.
5. Cady B, Rossi R. An expanded view of risk-group definition in differentiated thyroid carcinoma. Surgery. 1988. 104:947–953.
6. DeGroot LJ, Kaplan EL, McCormick M, Straus FH. Natural history, treatment, and course of papillary thyroid carcinoma. J Clin Endocrinol Metab. 1990. 71:414–424.
7. Hay ID, Bergstralh EJ, Goellner JR, Ebersold JR, Grant CS. Predicting outcome in papillary thyroid carcinoma: development of a reliable prognostic scoring system in a cohort of 1779 patients surgically treated at one institution during 1940 through 1989. Surgery. 1993. 114:1050–1057.
8. Mazzaferri EL, Jhiang SM. Long-term impact of initial surgical and medical therapy on papillary and follicular thyroid cancer. Am J Med. 1994. 97:418–428.
9. Sherman SI, Brierley JD, Sperling M, Ain KB, Bigos ST, Cooper DS, Haugen BR, Ho M, Klein I, Ladenson PW, Robbins J, Ross DS, Specker B, Taylor T, Maxon HR 3rd. National Thyroid Cancer Treatment Cooperative Study Registry Group. Prospective multicenter study of thyrois carcinoma treatment: initial analysis of staging and outcome. Cancer. 1998. 83:1012–1021.
10. Greene FL. The American Joint Committee on Cancer: updating the strategies in cancer staging. Bull Am Coll Surg. 2002. 87:13–15.
11. Schemper M. The relative importance of prognostic factors in studies of survival. Stat Med. 1993. 12:2377–2382.
12. Brierley JD, Panzarella T, Tsang RW, Gospodarowicz MK, O'Sullivan B. A comparison of different staging systems predictability of patient outcome. Thyroid carcinoma as an example. Cancer. 1997. 79:2414–2423.
13. Passler C, Prager G, Scheuba C, Kaserer K, Zettinig G, Niederle B. Application of staging systems for differentiated thyroid carcinoma in an endemic goiter region with iodine substitution. Ann Surg. 2003. 237:227–234.
14. Lang BH, Chow SM, Lo CY, Law SC, Lam KY. Staging systems for papillary thyroid carcinoma: a study of 2 tertiary referral centers. Ann Surg. 2007. 246:114–121.
15. Lang BH, Lo CY, Chan WF, Lam KY, Wan KY. Staging systems for papillary thyroid carcinoma: a review and comparison. Ann Surg. 2007. 245:366–378.
 XML Download
XML Download