

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The effects of testosterone are mediated by the androgen receptor (AR). The AR gene is located on Xq11-12 and consists of 8 exons. There are CAG repeats in the N-terminal of exon 1 of the AR gene. The number of CAG repeats has polymorphism ranging between 19 and 25 in Caucasian men [1-3]. It has been demonstrated that the number of CAG repeats in the AR gene inversely correlates with transcriptional activities [4]. Patients with Kennedy's disease have extreme CAG repeat lengths (> 40) and show androgen insensitivity [5,6]. The association between the number of CAG repeats and testosterone effects has been investigated with conflicting results. In healthy men, the CAG repeat length has shown positive correlation with body fat and high-density lipoprotein (HDL) cholesterol and negative correlation with triglyceride [3,7,8]. The CAG repeat length has been reported to have an association with serum testosterone level [8,9], impaired spermatogenesis and male infertility [10,11]. However, some studies have suggested that the number of CAG repeats has no association with height, weight, waist circumference, body fat [2,8,12], lipid profile [2] or serum testosterone levels [7,13].
In hypogonadal men, testosterone replacement improves sexual function and quality of life, decreases body fat and increases lean body mass and bone mineral density (BMD) [14-17]. Based on the fact that CAG repeats are associated with testosterone effects, it is conceivable that the CAG repeat polymorphism can have an effect on testosterone therapy in hypogonadal men. Previous studies have reported that CAG repeat length is associated with increased hematocrit and benign prostate hyperplasia (BPH) risk - an adverse effect of testosterone therapy in hypogonadal men [18,19].
The aim of this study was to investigate the association between the number of CAG repeats and the effect/safety of testosterone therapy in Korean hypogonadal men.
MATERIALS AND METHODS
1. Patients
This is a retrospective study. Forty-two patients who were diagnosed with hypogonadism and had testosterone replacement therapy at Seoul National University Hospital between December 1999 and August 2007 were included. The mean age of the patients was 45 years (range, 21-67). The mean body mass index (BMI) was 26.3 kg/m2. Before testosterone therapy, patients showed hypogonadism-related symptoms, such as loss of libido and their serum testosterone levels in the morning were under 200 ng/dL. Forty-one patients had secondary hypogonadism and only 1 patient had primary hypogonadism. There were 26 subjects with pituitary adenoma, 9 subjects with craniopharyngioma, 3 subjects with germinoma, 2 subjects with Rathke's cleft cyst, 1 subject with meningioma, and 1 subject with Klinefelter syndrome. Of these patients, 39 (71%) took glucocorticoid and 29 (69%) took levothyroxine. The data of 12 of the 41 patients who were included in this report were also included in our previous report [20,21].
Patients took oral testosterone (testosterone undecanoate, Andriol®, Organon, Seoul, Korea). Testosterone therapy was started from 40 mg twice a day (80 mg/day), and the dosage was titrated according to symptom severity such as a decrease in sex drive, a lack of energy, a decrease in strength and difficulties in erection. The mean final dosage of testosterone was 80 mg twice a day (160 mg/day; range, 80-240 mg/day). This study protocol was approved by the Institutional Review Board of the Seoul National University Hospital.
2. Measurement of body composition and bone mineral density
Height, weight, lean body mass, body fat, and the result of BMD before testosterone therapy and at the 12-month and 24-month follow-up were identified by our review of the medical records. BMI was calculated by the Qutelet's formula: BMI = weight (kg)/height (m)2. Lean body mass and body fat were measured by using a bioelectric impedance analyzer (Inbody 3.0, Biospace, Seoul, Korea). BMD at the lumbar spine and femoral neck was measured using a dual energy X-ray absorptiometer (DXA, GE LUNAR, Madison, WI, USA) in 26 patients at 12-month follow-up and in 19 patients at 24-month follow-up were measured.
3. Biochemical analysis
The results of blood samples before testosterone therapy and at the 12-month and 24-month follow-up were identified by our review of the medical records in terms of testosterone, total cholesterol, triglyceride, HDL cholesterol, hemoglobin, hematocrit, prostate-specific antigen (PSA), serum osteocalcin and urine type I collagen N-telopeptide (NTx). Serum testosterone levels were measured using an immunoradiometric assay kit (Siemens, Erlangen, Germany). Low-density lipoprotein (LDL) cholesterol was calculated by the Friedwald equation when triglyceride was under 400 mg/dL: total cholesterol - (triglyceride/5 + HDL cholesterol).
4. Determination of the number of CAG repeats in the androgen receptor gene
Genomic DNA was isolated from ethylenediaminetetraacetic acid (EDTA) blood samples using a blood DNA kit (Gentra, Minneapolis, MN, USA). DNA was stored at -80℃ until analyzed. The exon 1 of the AR gene was amplified by polymerase chain reaction (PCR). The final volume of the reaction sample was 50 µL, consisting of buffer 10 × 5 µL, deoxynucleotide triphosphate 4 µL, primer 1 µL, Taq polymerase 0.5 µL (Takara, Shiga, Japan) and DNA 1 µL. The primer sequences were 5'-GCCTGTTGAACTCTTCTGAGC-3' and 5'-CGATGGGCTTGGGGAGAACCATCCTCA-3'. PCR reaction was cycled at 94℃ for 2 minute; 35 cycles of 94℃ for 50 second, 58℃ for 40 second and 72℃ for 1 minute; and 72℃ for 10 minute. PCR product was electrophoresed in 1.2% agarose gel and was extracted by a QIAquick Gel Extraction kit (Quiagen, Hilden, Germany). The number of CAG repeats in the AR gene was determined by direct sequencing.
5. Statistical analysis
All data are expressed as mean ± standard deviation. The correlation between the dosage of oral testosterone and the number of CAG repeats was examined with Spearman's correlation. The paired t-test was used to compare parameters before and after testosterone therapy. The patients were divided into 4 quartiles according to the number of CAG repeats: Q1, 15-21 (n = 11), Q2, 22-23 (n = 12), Q3, 24-25 (n = 9) and Q4, 26-29 (n = 10). The Kruskall-Wallis test was used to compare the 4 groups. Correlation coefficients between changes in parameters after testosterone therapy and the number CAG repeats were determined using Spearman's correlation. SPSS (version 15.0; SPSS, Chicago, IL, USA) was used for all statistical analyses. A P value of < 0.05 was considered statistically significant.
RESULTS
The mean oral testosterone dosage used was 160 mg/day. Neither final dosage of testosterone nor cumulative dosage of testosterone showed the correlation with the number of CAG repeats (r = -0.092, P = 0.156; r = -0.143, P = 0.366). The mean serum testosterone levels before testosterone therapy were 45.8 ± 63.3 ng/dL. Serum testosterone levels could be indentified in 33 patients 24 months after testosterone therapy and increased from 45.8 ng/dL to 116.3 ng/dL.
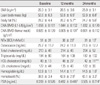
BMI, body composition, BMD, bone turnover markers, hematocrit, and PSA before and after testosterone therapy are shown in Table 1. BMI did not change during testosterone therapy. However, mean lean body mass increased from 51.7 kg before testosterone therapy to 52.8 kg at 12 months and to 52.9 kg at 24 months (P < 0.01). Mean body fat decreased from 28.2% before testosterone therapy to 26.2% at 12 months and to 24.7% at 24 months (P < 0.01). A slight decrease in BMD was observed at the femoral neck at 12 months, but it was statistically insignificant at 24 months. NTx decreased from 51 BCE/mMolCr before testosterone therapy to 36 BCE/mMolCr at 12 months and to 33 BCE/mMolCr at 24 months (P < 0.01). There were no significant differences in lipid profiles except HDL cholesterol. Mean HDL cholesterol decreased from 49 mg/dL to 42 mg/dL at 24 months (P < 0.01). Hemoglobin, hematocrit and PSA increased significantly during testosterone therapy (P < 0.01). However, none of the patients had hemoglobin more than 17.0 g/dL and hematocrit more than 50%. None of the patients discontinued the testosterone therapy because of elevated PSA (> 3.0 ng/mL), newly developed BPH related symptoms, aggravated BPH or newly developed prostate cancer.
The mean number of CAG repeats was 23 ± 3 (range, 15-29). Baseline characteristics were assessed according to the number of CAG repeats (Table 2). There were no significant differences in parameters except BMI between the quartile groups. BMI showed a significant increase as the number of CAG repeats increased (P < 0.05).
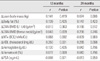
We evaluated the associations between the number of CAG repeats and lean body mass, body fat, NTx, HDL cholesterol, hematocrit or PSA, all of which showed significant changes after testosterone therapy. The number of CAG repeats was not correlated with changes in lean body mass, body fat, NTx, HDL cholesterol, hematocrit and PSA during testosterone therapy (Table 3). As the number of CAG repeats in the AR gene increased, HDL cholesterol decreased at 12 months (r = 0.350, P = 0.031), but the difference was not statistically significant at 24 months. Changes in lean body mass, body fat, NTx, HDL cholesterol, hematocrit and PSA during testosterone therapy with reference to the quartiles of the CAG repeats did not show any significant differences (Fig. 1).
DISCUSSION
In this study, 24 months of testosterone replacement therapy increased lean body mass, hematocrit and PSA, and decreased body fat, NTx and HDL cholesterol. The results of this study correspond with those of previous studies which reported that testosterone therapy improves lean body mass and body fat, but the effects of testosterone therapy on BMI were not consistent [17,22]. While NTx decreased continuously during testosterone therapy, BMD did not improve in this study. This may be explained by the fact that BMD was measured only in 26 patients (62%) at 12 months and in 19 patients (45%) at 24 months and that the follow-up duration was short. The number of CAG repeats in the AR gene is known to differ between ethnic groups. The mean of the number of CAG repeats in Asians was 22-23, and it was slightly higher than that in Caucasians [23,24]. In the present study with Korean men, the number of CAG repeats was similar to those of previous report [24].
Testosterone therapy improves sexual function and quality of life, and it increases lean body mass and BMD. However, it can increase hematocrit and the risk of prostate cancer or BPH. If there is a factor which can predict the effect and adverse reactions of testosterone, it can give useful information to decide on testosterone therapy in hypogonadal patients. Zitzmann and Nieschlag [18,25] have documented that the number of CAG repeats in hypogonadal patients is associated with increased hematocrit and risk of BPH. Therefore, we investigated the association between the number of CAG repeats and the effect/safety of testosterone therapy in Korean hypogonadal men. However, it has been demonstrated that the number of CAG repeats is not associated with changes in lean body mass, body fat, NTx, HDL cholesterol, hematocrit and PSA during testosterone therapy. There was no association even when the patients were divided into 4 quartiles according to the number of CAG repeats. One reason for the discrepancy between Zitzmann's report and ours may be the difference in study subjects. In our study, most subjects had secondary hypogonadism in contrast to Zitzmann's study which include subjects with primary hypogonadism as well as those with secondary hypogonadism. Some patients with secondary hypogonadism may have both hypogonadism and another hormone deficiency. In this study, about 70% of patients took glucocorticoid or levothyroxine due to hypopituitarism. Glucocorticoid can increase body fat, cause weight gain and reduce bone density. However, there were no significant differences between glucocorticoid users and nonusers in changes in BMD during testosterone therapy (data not shown). Second, the number of CAG repeats was different (21 ± 4 [range, 13-30] vs. 23 ± 3 [range, 15-29]), which may be due to a racial difference. Another reason may be the difference in study methods. We only measured PSA, while previous studies used ultrasonography to assess an increased risk of BPH [18,19,25]. In Zitzmann's study, the number of CAG repeats was associated with PSA, but not with prostate volume [18]. However, conflicting results have been reported about the association between the number of CAG repeats and BPH [26]. Furthermore, controversy exists regarding the association between testosterone therapy and prostate-related events such as BPH and prostate cancer [27]. Therefore, additional studies are needed to determine the association between the number of CAG repeats and BPH or prostate cancer.
This study has clinical implications in that it is the first study performed in Asia to investigate the importance of AR gene CAG repeat polymorphism in the effect and safety of testosterone therapy. However, this study has some limitations. First, the number of subjects was small and follow-up duration was relatively short. Second, the dosage of oral testosterone used was different between patients and serum testosterone levels were lower than normal, although serum testosterone levels increased after testosterone therapy. This suggests that testosterone may be insufficient. However, because oral testosterone has a short duration of action and the bioavailability of oral testosterone is greatly affected by food, serum testosterone levels can be low even in optimal dosage [28,29]. The serum testosterone level is known to reach a peak 2-6 hours after administration of oral testosterone and return to baseline within 24 hours [29].
In conclusion, the results of this study suggest that the number of CAG repeats may be not associated with changes in lean body mass, body fat, NTx, HDL cholesterol, hematocrit and PSA during testosterone therapy.


 XML Download
XML Download