

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Insulin resistance has been accepted as the most important factor in describing the pathophysiology of the metabolic syndrome (MetS), which has been increasingly identified worldwide in association with the epidemic of obesity [1-3]. This syndrome is characterized by well-known risk factors for cardiovascular disease (CVD), such as glucose intolerance, hypertension, dyslipidemia and central obesity. Although body mass index (BMI) is the most widely used surrogate reflecting obesity and is reliably associated with adverse metabolic outcomes, it does not necessarily correlate with the degree of insulin resistance.
Recent observations indicate that a subgroup of nonobese or slightly obese subjects who are metabolically obese but normal weight (MONW) individuals, present with several risk factors in relation to insulin resistance [4,5]. Persons with MONW are characterized by an altered insulin sensitivity, a higher level of abdominal and visceral adiposity, a more atherogenic lipid profile, a higher blood pressure and a lower physical activity energy expenditure, thus being more vulnerable to type 2 diabetes and CVD [5-11]. Somewhat the opposite of MONW individuals are metabolically healthy but obese (MHO) individuals who demonstrate normal to high levels of insulin sensitivity, a lower level of visceral adiposity and more favorable cardiovascular risk profiles despite having large amounts of fat mass [5,12-14].
Asian populations are generally less obese but tend to have hi-gher body fat content and a higher degree of insulin resistance than other ethnic populations with similar BMI [15-17]. Although identifying subgroups of MONW or MHO might have clinical significance, studies on Asian subjects have been rarely conducted [8,18]. Therefore, we aimed to identify the prevalence and the clinical characteristics of MONW and MHO individuals in a large cohort of the middle-aged non-diabetic Korean population. Also, their relevance to diabetes and the risk of coronary heart disease (CHD) were investigated.
MATERIALS AND METHODS
1. Subjects
This population-based cohort study was performed in 2003-2006 on adults over 40 years old living in the rural area of Chungju city, Korea. Three hundred and thirty-four districts were selected by stratified random cluster sampling and 11,718 subjects participated. We analyzed the data of 8987 subjects (3632 men and 5355 women) who were without known or newly diagnosed diabetes mellitus, with complete laboratory data including fasting insulin, as well as anthropometric measurement. This study was approved by the institutional review board of The Catholic University of Korea (No. CUMC10U941, CUMC10U942) and written informed consent was obtained from all participants.
2. Protocols and biochemical assays
All investigators were educated sufficiently in relation to the study protocol prior to physical examination and the questionnaire. On the day of the investigation, the detailed data on the medical history, medication and smoking habits of the subjects were obtained. Physical examinations were performed by measuring height, weight, waist and hip circumference according to standardized methods. Prior to the measurement of blood pressure (BP), the subjects were asked to rest for 5 minutes while seated. The BP on the right upper arm was measured twice and the average of two measurements was obtained. Blood samples were collected after the subjects had fasted for at least 12 hours and analysed at a central laboratory (Samkwang Medical Laboratories, Seoul, Korea). Fasting plasma glucose (FPG) was measured using the hexokinase method and serum insulin was measured using a radioimmunoassay kit (Dainabot, Tokyo, Japan). Serum total cholesterol and triglyceride (TG) were measured using enzymatic calorimetric tests, high-density lipoprotein (HDL) cholesterol was measured using a selective inhibition method, and low-density lipoprotein (LDL) cholesterol was calculated by Friedewald formula. A 75 g oral glucose tolerance test (OGTT) was performed on a separate day if the FPG level exeeded 110 mg/dL. Other study protocols, including the method of measuring anthropometry and blood pressure, have been described in detail in our previous reports [19-21].
3. Definition of metabolic syndrome and prediabetes
MetS was defined using the American Heart Association/National Heart, Lung and Blood Institute criteria with a modification in waist circumference (WC) value according to the World Health Organization-Asian Pacific region criteria for abdominal obesity [22]. It was defined if three or more of the following criteria were satisfied: 1) WC ≥ 90 cm for men and ≥ 80 cm for women; 2) TG ≥ 150 mg/dL; 3) HDL-cholesterol < 40 mg/dL for men and < 50 mg/dL for women; 4) BP ≥ 130/85 mmHg or 5) FPG ≥ 100 mg/dL. All individuals taking pharmacological treatment for hypertension were assumed as having raised BP and all subjects receiving fibrates were assumed as having both raised TG and reduced HDL-cholesterol. Diabetes and prediabetes were defined according to the American Diabetes Association criteria. As the OGTT was performed in subjects with abnormal FPG, prediabetes included subjects with isolated impaired fasting glucose or combined impaired fasting glucose and impaired glucose tolerance.
4. Definition of metabolically healthy and normal weight (MHNW), MONW, MHO and metabolically obese and obese (MOO)
Being 'metabolically obese' was defined as having the highest quartile of insulin resistance estimated by the homeostasis model assessment (HOMA-IR = fasting insulin [µU/mL] × FPG [mmol/L]/22.5) [23]. Being 'metabolically healthy' was defined as having the lowest quartile of HOMA-IR. MHNW and MONW were defined if individuals had a BMI ≥ 18.5 and < 23 kg/m2 with HOMA-IR in the lowest and highest quartile, respectively. MHO and MOO were defined if individuals had a BMI ≥ 25 kg/m2 with HOMA-IR in the lowest and highest quartile, respectively. Another definition was also adopted, where having MetS was defined as 'metabolically obese' and not having MetS as 'metabolically healthy' (MetS derived definition).
5. Assessment of CHD risk
The Framingham risk score was used in predicting the likelihood of CHD during the following 10-year period [24]. The degrees of risk were converted to numerical values based on factors including age, diabetes, smoking habit, BP, TC or LDL-cholesterol levels and HDL-cholesterol levels, and were expressed as percentile values.
6. Statistical analysis
All statistical analyses were performed using SAS version 9.01 package (SAS institute, Cary, NC, USA). Parameters showing skew-ed distributions (insulin, HOMA-IR, TG) were transformed logarithmically to achieve a normal distribution. The differences in the characteristics of subgroups were compared using Student's t tests or Chi squared tests. Analysis of covariance was used to compare the age-adjusted 10-year risk of CHD among the subgroups. Data are expressed as the means ± standard deviation (SD), as medians (25th-75th percentiles) or in percentile values except where noted. A P-value < 0.05 was considered significant.
RESULTS
1. Baseline characteristics
The baseline clinical characteristics are shown in Table 1. The mean age of the participants was 62.3 ± 10.5 years and 40.4% were male. The mean BMI, WC and waist-hip ratio (WHR) of the men were 23.4 ± 3.1 kg/m2, 84.1 ± 8.4 cm and 0.92 ± 0.06, respectively. In women, the mean values of these parameters were 24.6 ± 3.4 kg/m2, 81.4 ± 8.9 cm and 0.88 ± 0.07, respectively. The prevalence of prediabetes (20.4 vs. 14.9%, P < 0.0001) was higher in men, while hypertension (49.8 vs. 45.7%, P < 0.0001) and metabolic syndrome (40.0 vs. 22.9%, P < 0.0001) were more frequent in women. As all of the parameters except age and BP were significantly different between men and women, further analyses were performed separately.
2. The prevalence of MONW and MHO
Table 2 shows the distribution of the subjects according to HOMA-IR quartile and BMI groups. The prevalence of MONW was 5.95% for men and 3.96% for women. This corresponds to 14.2% for men and 12.9% for women, among the normal weight subjects. The prevalence of MHO was 3.08% for men and 6.14% for women. This corresponds to 10.7% for men and 14.5% for women among obese subjects. The prevalence of MONW increased in proportion to age while that of MHO decreased both in men and women (Fig. 1). The age-adjusted prevalence of MONW and MHO were 4.3% (95% confidence interval [CI]: 3.8, 4.9) (5.3% [95% CI: 4.4, 6.3] for men, 3.7% [95% CI: 3.1, 4.3] for women) and 5.6% (95% CI: 5.0, 6.3) (3.6% [95% CI: 2.7, 4.5] for men, 7.0% [95% CI: 6.0, 7.9] for women), respectively. Using the MetS derived definition, the prevalence of MONW were 3.73% for men (8.9% among normal weight subjects) and 6.94% for women (22.7% among normal weight subjects). In this case, the prevalence of MHO were 15.2% for men (52.8% among obese subjects) and 18.9% for women (44.4% among obese subjects).
3. The comparison of subgroups according to HOMA-IR quartile and BMI groups
Table 3 shows the comparison between subjects with MHNW versus MONW, MHO versus MOO, and MONW versus MHO in men. The age was generally higher in the normal weight group than the obese group. Within the same BMI group, subjects within the highest quartile of insulin resistance (MONW and MOO) had significantly higher levels of BMI, WC, WHR, FPG, fasting insulin, HOMA-IR, and lipid profiles than the subjects within the lowest quartile of insulin resistance (MHNW and MHO). When comparing MONW with MHO, FPG, fasting insulin, and HOMA-IR of MONW were significantly higher than those of MHO. However, diastolic BP was significantly higher in MHO and there were no significant differences in lipid profiles (Table 3). Similar results were noted in women (Table 4). Additionally, the TG levels of MONW were higher than those of MHO. The prevalence of prediabetes and metabolic syndrome was significantly higher in MONW and MOO groups when compared to the MHNW and MHO groups, respectively. Despite a lesser degree of obesity, when compared with MHO group, subjects within MONW group showed a higher prevalence of prediabetes (34.7 vs. 12.5%, P < 0.0001 in men; 23.1 vs. 8.8%, P < 0.0001 in women). However, there were no significant differences in the prevalence of hypertension between the two groups. These findings were similar in men and women (Fig. 2).
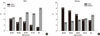
4. Estimated age-adjusted 10-year CHD risk
Within the same BMI group, subjects within the highest quartile of insulin resistance (MONW and MOO) had a significantly higher risk of CHD than the subjects within the lowest quartile of insulin resistance (MHNW and MHO). The risk of CHD was highest in MOO group and showed significant differences when compared with the other three groups. The MONW group showed an equivalent risk of CHD when compared with the MHO group (10.77 ± 0.68 vs. 10.22 ± 0.90% in men; 7.02 ± 0.34 vs. 7.26 ± 0.26% in women, means ± standard error [SE]). These findings were similar in men and women (Fig. 3). However, using the MetS derived definition, the 10-year CHD risk of the MONW group was significantly higher than that of the MHO group in both men (22.48 ± 0.80 vs. 8.98 ± 0.38%, P < 0.0001) and women (10.34 ± 0.25 vs. 4.82 ± 0.13%, P < 0.0001).
DISCUSSION
In general, it is known that the more obese an individual, the more likely they are to be insulin resistant. However, subphenotypes of obesity have been recognized that diverge from this association. Since the proposal of the concept of MONW and MHO, several studies had been performed on the prevalence and clinical characteristics of these subjects [4-14]. Although Asian populations show significant differences in the distribution of obesity and the degree of insulin resistance, there is little information available on these subphenotypes. Our data show that a substantial proportion of people could be classified as MONW or MHO and emphasizes the necessity of our attention. Despite a lesser degree of obesity, subjects within MONW group showed a higher prevalence of prediabetes and at least an equivalent risk of CHD when compared with the MHO group.
Previous studies demonstrated that the prevalences of MONW and MHO vary considerably according to the subjects and the various definitions used. The prevalence of MONW ranged from 4.6 to 23.5% of the normal weight population; however, such studies mainly included Caucasians. Park et al. [25] reported from the third National Health and Nutrition Examination Survey (NHANES) that 4.6% of men and 6.2% women with BMI less than 27 kg/m2 had MetS. Meigs et al. [11] demonstrated that 7% and 7.7% of subjects with BMI less than 25 kg/m2 had MetS or highest quartile of HOMA-IR, respectively. Despite the higher BMI criteria used, these studies showed a lower prevalence of MONW than our observations, which might imply ethnic differences. Twenty three point five Percent of US adults with BMI less than 25 kg/m2 had more than 2 cardiometabolic abnormalities, such as elevated BP, elevated levels of TG, FPG, and high-sensitivity C-reactive protein, elevated HOMA-IR value and reduced HDL-cholesterol level [26]. To date, there is only one Korean data set showing that 12.7% of adults with BMI less than 25 kg/m2 had MetS, from the third Korean NHANES [18]. Although this study adopted different diagnostic criteria, it suggests that more than 10% of Korean normal weight subjects could be classified as MONW, which seems to be in conjunction with our study. The prevalence of MHO is also highly variable but tends to be higher than that of MONW especially when the absence of MetS is considered as being 'metabolically healthy'. Meigs et al. [11] reported that 37% of subjects with BMI over 30 kg/m2 did not have MetS and Wildman et al. [26] demonstrated that 31.7% of adults with BMI over 30 kg/m2 had no, or only one, cardiometabolic abnormality. The Korean NHANES data showed that nearly half (47.9%) of the obese (BMI ≥ 25 kg/m2) subjects did not have MetS [18]. When using the same criteria, the prevalence of MHO in our subjects was similar. However, it was greatly reduced when adopting HOMA-IR criteria. The age-dependent increase in the prevalence of MONW and decrease in that of MHO is consistent with previous observations [11,18,26] and might be associated with an increase in the degree of insulin resistance and the loss of lean mass that occurs with the aging process [27].
Several well-known characteristics of MONW were identifiable, including central obesity, increased FPG levels and a more atherogenic lipid profile when compared with subjects with MHNW. Opposite findings characterized MHO compared with MOO. Interestingly, subjects within the MONW group showed a higher prevalence of prediabetes and an equivalent risk of CHD when compared with the MHO group, in spite of a lesser degree of obesity. When regarding having MetS as being 'metabolically obese', the risk of CVD was significantly higher in the MONW group compared to that of the MHO group. These results suggest that subjects with MONW is prone to at least an equivalent risk of CHD compared with subjects with MHNW, although it may vary according to different definitions used. Obesity is one of the important factors contributing to insulin resistance that results in the development of CVD and type 2 diabetes [28,29]. However, as most obese people do not experience such cardiometabolic diseases, insulin resistance, rather than simple obesity, might be serving as a core pathophysiologic mechanism. In fact a meta-analysis of 250,152 patients with CHD found that obese (BMI 30-35 kg/m2) patients had no increased risk for total mortality or cardiovascular mortality [30]. Another point to consider is whether differences in clinical characteristics of MONW and MHO will really result in corresponding clinical outcomes. One longitudinal study following subjects up to 11 years showed that the MONW group had a relative risk for diabetes of 3.97 (95% confidence interval 1.35-11.6) and a risk for CVD of 3.01 (1.68-5.41) [11]; however, more evidence should be accumulated. Whether MHO individuals would gain any metabolic benefit from lifestyle modification and weight loss also remains to be elucidated, since a few studies have failed to demonstrate metabolic improvements after intervention [31].
A strength of our study is that these data come from the largest population with homogenous ethnicity and similar lifestyle patterns. However, this study has several limitations. Because this cohort consists of middle-aged to elderly subjects, the prevalence and the characteristics might be somewhat different when younger individuals are included. We could not measure the body fat mass, energy expenditure or the levels of adipokines which might further characterize the subgroups of subjects. In addition, the method of measuring the degree of insulin resistance was not the gold standard, although HOMA-IR is a suitable measure for large-scale studies and is a good representative in non-diabetic subjects. We also have to consider that the application of Framingham CHD risk score in Koreans is not validated yet.
In conclusion, when MONW and MHO were defined by BMI category and HOMA-IR quartiles, the prevalence of these subgroups in Korea was not negligible. More than 10% of normal weight subjects were classified as MONW and similar proportions of obese subjects belonged to MHO. The subjects in MONW group are confronted by a high risk of diabetes and CHD despite their normal weight. Future studies should focus upon finding easier and more precise markers for MONW and MHO. In addition, the mechanisms and genetic background that might explain the differences in the characteristics should be further investigated. Developing a consensus on the criteria for definition of these subgroups is an important issue and will broaden our understanding regarding the clinical importance of MONW and MHO.






 XML Download
XML Download