

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Background
It is uncommon to unexpectedly discover pituitary tumor as a hypermetabolic lesion on an 18F-FDG PET-CT scan for the evaluation of an unrelated disease when the patient does not show neurological or endocrine signs and symptoms.
Methods
We retrospectively analyzed the medical records of 16 patients with pituitary tumor that was detected incidentally on 18FFDG PET-CT at the Korea Cancer Center Hospital from January 2002 to September 2009. We analyzed their clinical features in detail.
Results
On 35,505 18F-FDG PET-CT scans, 16 (0.045%) patients were diagnosed with pituitary incidentaloma. They underwent 18FFDG PET-CT for the evaluation of the state of malignancy. All of them had no signs and symptoms related to pituitary tumor. The average age of the patients was 63.3 ± 12.0 years (49-85 years). Eleven patients were men and 5 were women. The mean diameter of the tumor was 17.9 ± 5.7 mm. Most of the pituitary incidentalomas were macroadenoma. The result of tumor morphologic evaluation by the Hardy classification was as follows: 6 grade IV, 1 grade III, 3 grade II and 1 grade I. The mean standardized uptake value of the tumor was 10.6 ± 6.7. Ten patients had endocrine evaluation and they showed a normal hormone level. Among 16 patients, 4 patients received TSA and they were diagnosed with pituitary adenoma.
Figures and Tables
 | Fig. 1Midline sagittal section (A) and coronal section (B) of 18FDG-PET. Focal FDG uptake at the pituitary gland (arrow).
|
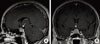 | Fig. 2Midline sagittal (A) and coronal (B) image of gadolinium-enhanced T1 weighted MRI. 19 × 17 × 15 mm heterogeneously enhanced mass involving pituitary gland (arrow).
|


References
1. Kim DY. The application of PET-CT in oncology. J Kyung Hee Univ Med Cent. 2005. 21:10–19.
2. Donovan LE, Corenblum B. The natural history of the pituitary incidentaloma. Arch Intern Med. 1995. 155:181–183.
3. Liao AC, Wan SC, Tsai F, Chen YK, Shen YY. Incidental pituitary macroadenoma detected in FDG-PET: three cases report. Ann Nucl Med Sci. 2002. 15:211–217.
4. Campeau RJ, David O, Dowling AM. Pituitary adenoma detected on FDG positron emission tomography in a patient with mucosa-associated lymphoid tissue lymphoma. Clin Nucl Med. 2003. 28:296–298.
5. Lee JH, Han SJ, Park SE, Cho MA, Cheong JW, Yun M, Rhee Y, Lee EJ, Lim SK. Non-functional pituitary adenoma detected on 18F-fluorodeoxyglucose positron emission tomography (18F-FDG-PET) in a patient with mucosa-associated lymphoid tissue lymphoma. J Korean Endocr Soc. 2008. 23:137–141.
6. Song YM, Lim DJ, Moon SD, Han JH, Han CW, Kim SH. A non-functioning pituitary macroadenoma detected incidentally with PET-CT. Korean J Med. 2009. 76:374–379.
7. Wilson CB. A decade of pituitary microsurgery. The Herbert Olivecrona lecture. J Neurosurg. 1984. 61:814–833.
8. Molitch ME, Russell EJ. The pituitary "incidentaloma". Ann Intern Med. 1990. 112:925–931.
9. Teramoto A, Hirakawa K, Sanno N, Osamura Y. Incidental pituitary lesions in 1,000 unselected autopsy specimens. Radiology. 1994. 193:161–164.
10. Wolpert SM, Molitch ME, Goldman JA, Wood JB. Size, shape and appearance of the normal female pituitary gland. AJR Am J Roentgenol. 1984. 143:377–381.
11. Hall WA, Luciano MG, Doppman JL, Patronas NJ, Oldfield EH. Pituitary magnetic resonance imaging in normal human volunteers: occult adenomas in the general population. Ann Intern Med. 1994. 120:817–820.
12. Lee YJ, Cho SW, Kim SW, Shin CS, Park KS, Cho BY, Lee HK, Kim SY. Characteristics and natural course of pituitary incidentaloma in Korea. J Korean Endocr Soc. 2008. 23:111–116.
13. Francavilla TL, Miletich RS, DeMichele D, Patronas NJ, Oldfield EH, Weintraub BD, Di Chiro G. Position emission tomography of pituitary macroadenomas: hormone production and effects of therapies. Neurosurgery. 1991. 28:826–833.
14. Reincke M, Allolio B, Saeger W, Menzel J, Winkelmann W. The 'incidentaloma' of the pituitary gland. Is neurosurgery required? JAMA. 1990. 263:2772–2776.
15. Sanno N, Oyama K, Tahara S, Teramoto A, Kato Y. A survey of pituitary incidentaloma in Japan. Eur J Endocrinol. 2003. 149:123–127.
16. Juweid ME, Cheson BD. Positron-emission tomography and assessment of cancer therapy. N Engl J Med. 2006. 354:496–507.
17. Kang KW. Combined PET/CT in oncology. Korean J Nucl Med. 2002. 36:80–86.
18. Soret M, Bacharach SL, Buvat I. Partial-volume effect in PET tumor imaging. J Nucl Med. 2007. 48:932–945.
19. Muhr C, Bergstrom M. Positron emission tomography applied in the study of pituitary adenomas. J Endocrinol Invest. 1991. 14:509–528.
20. Bonneville JF, Bonneville F, Cattin F. Magnetic resonance imaging of pituitary adenomas. Eur Radiol. 2005. 15:543–548.
21. Bergström M, Muhr C, Lundberg PO, Långström B. PET as a tool in the clinical evaluation of pituitary adenomas. J Nucl Med. 1991. 32:610–615.
22. Tang BN, Levivier M, Heureux M, Wikler D, Massager N, Devriendt D, David P, Dumarey N, Corvilain B, Goldman S. 11C-methionine PET for the diagnosis and management of recurrent pituitary adenomas. Eur J Nucl Med Mol Imaging. 2006. 33:169–178.
23. Alzahrani AS, Farhat R, Al-Arifi A, Al-Kahtani N, Kanaan I, Abouzied M.
. Pituitary. 2009. 12:309–314.
 XML Download
XML Download