

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
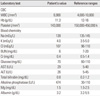
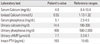
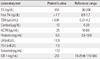
Pseudohypoparathyroidism is a rare disease that is characterized by target cell resistance to the effects of parathyroid hormone and this disease is classified into various types depending on the phenotypic and biochemical findings. The patients with pseudohypoparathyroidism present with the clinical and biochemical features of hypoparathyroidism, but they have an increased serum level of parathyroid hormone. We experienced a case of pseudohypoparathyroidism in a 24 years old woman who had Graves' disease at that time. She had hypocalcemia, hyperphosphatemia, an elevated serum parathyroid hormone level and a normal urinary basal cyclic AMP(adenosine monophosphate) level. She also had a normal phenotypic appearance. Therefore, she was classified as suffering with pseudohypoparathyroidism type II. The clinical and laboratory abnormalities were improved by calcium supplementation in addition to vitamin D. To the best of our knowledge, this is the first case of pseudohypoparathyroidism combined with Graves' disease in Korea.


References
1. Albright F, Burnett CH, Smith PH, Parson W. Pseudohypoparathyroidism--an example of the "seabright-bantam syndrome". Endocrinology. 1942. 30:922–932.
2. Lee Y, Roh J, Yoo JS, Han J, Nam J, Cho M, Park J, Ahn C, Kim K. A case of pseudohypoparathyroidism without albright's hereditary osteodystrophy in an adult. J Korean Endocr Soc. 2009. 24:132–137.
3. Lee IS, Kim YJ, Choi YS, Kim SY, Lee YH, Jo YS, Shong M. Two cases of pseudohypoparathyroidism in sisters. Korean J Med. 2008. 74:S209–S216.
4. Kang MI, Park YB, Lee YG, Yoo SJ, Son HS, Yoon KH, Hong KS, Lee KW, Son HY, Kang SK, Kim BS. Pseudohypoparathyroidism type Ia and type II. J Korean Soc Endocrinol. 1991. 6:170–178.
5. Kim YS, Lee SH, Byun DI, Lee WK, Kim BH, Kim YH, Ko YS. A case of pseudohypoparathyroidism type I. J Korean Endocr Soc. 2006. 21:338–344.
6. Kim WJ, Moon SJ, Kim HY, Lee CB. A case of pseudohypoparathyroidism worsened by rhabdomyolysis. J Korean Endocr Soc. 2009. 24:195–200.
7. Ogata E, Yamamoto M, Matsumoto T, Fujita T, Fukase M, Kinoshita Y, Furukawa Y, Sohn HE, Nakajima H, Yasuda T. Standard procedure and the diagnostic criteria for the Ellsworth-Howard test using human PTH-(1-34). Nippon Naibunpi Gakkai Zasshi. 1984. 60:971–984. [Japanese].
8. Kim YS. Interpretation and reading of endocrine function test. 2001. 1st ed. Seoul: Korea Medical Book Publisher;116–118.
9. Spiegel AM, Gierschik P, Levine MA, Downs RW Jr. Clinical implications of guanine nucleotide-binding proteins as receptor-effector couplers. N Engl J Med. 1985. 312:26–33.
10. Farfel Z, Brickman AS, Kaslow HR, Brothers VM, Bourne HR. Defect of receptor-cyclase coupling protein in pseudohypoparathyroidism. N Engl J Med. 1980. 303:237–242.
11. Haussler MR, McCain TA. Basic and clinical concepts related to vitamin D metabolism and action (first of two parts). N Engl J Med. 1977. 297:974–983.
12. Bastepe M, Jüppner H. GNAS locus and pseudohypoparathyroidism. Horm Res. 2005. 63:65–74.
13. Farfel Z, Friedman E. Mental deficiency in pseudohypoparathyroidism type I is associated with Ns-protein deficiency. Ann Intern Med. 1986. 105:197–199.
14. Barrett D, Breslau NA, Wax MB, Molinoff PB, Downs RW Jr. New form of pseudohypoparathyroidism with abnormal catalytic adenylate cyclase. Am J Physiol. 1989. 257:E277–E283.
15. Linglart A, Carel JC, Garabédian M, Lé T, Mallet E, Kottler ML. GNAS1 lesions in pseudohypoparathyroidism Ia and Ic: genotype phenotype relationship and evidence of the maternal transmission of the hormonal resistance. J Clin Endocrinol Metab. 2002. 87:189–197.
16. Drezner M, Neelon FA, Lebovitz HE. Pseudohypoparathyroidism type II: a possible defect in the reception of the cyclic AMP signal. N Engl J Med. 1973. 289:1056–1060.
17. Holick MF. Vitamin D deficiency. N Engl J Med. 2007. 357:266–281.
18. Gerhardt A, Hackenberg K. Pseudohypoparathyroidism and Grave's disease: a rare combination of two endocrinological diseases. Exp Clin Endocrinol Diabetes. 2002. 110:245–247.
19. Uchimura H, Ariyama T, Wada K, Araki J, Kuwahata T. Proceedings: A case of pseudohypoparathyroidism with hyperthyroidism. Calcif Tissue Res. 1974. 15:161.
20. Hashimoto M, Tagami T, Shigemitsu M, Satoh N, Usui T, Yamada K, Shimatsu A, Kuzuya H, Sugawara A. Case of pseudo-hypoparathyroidism type II with Basedow's disease. Clin Calcium. 2004. 14:122–126. [Japanese].
 XML Download
XML Download