

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Non-islet cell tumor induced hypoglycemia (NICTH) is attributable to overproduction of insulin-like growth factor-II (IGF-II) by solid tumors, and these tumors usually originate from mesenchymal or epithelial cells. Gastrointestinal stromal tumor (GIST) is a rare mesenchymal tumor and most commonly find in the gastrointestinal tract. It is usually expresses the CD117 (stem cell factor receptor, c-kit) detected by immunohistochemistry. Hypoglycemia associated with GIST is very rare and this has not yet been reported in Korea. A 72-year-old man was hospitalized due to frequent episodes of confusion. It was observed that non-hyperinsulinemic hypoglycemia, an elevated serum IGF-II level and a huge liver mass. The histology of liver mass showed c-kit (CD117) positivity, which was consistent with GIST, but it was surgically unresectable. He was treated with imatinib mesylate. Although he recieved palliative treatment, he still experienced intermittent fasting hypoglycemia. After 2 months, the serum IGF-II level was even higher than before. We changed imatinib mesylate to sunitinib malate and performed radiotherapy on the liver mass. Although the change of the liver mass was not significant, he did not suffer from hypoglycemia for three months afterwards.
Figures and Tables
Fig. 1
Early-enhanced (A), delayed-enhanced (B) computerized tomographic images of the abdomen. A huge mass lesion is noted in the liver.
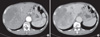
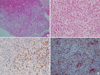
Fig. 2
A. Pathologic finding of liver mass is composed of spindle-shaped tumor cells (H&E stain, × 100). B. Some mitoses were identified. The mitotic count was up to 16/10 high power field (H&E stain, × 400). C. C-kit immunohistochemical stain was positive. D. CD34 immunohistochemical stain was positive.
References
1. Marks V, Teale JD. Tumours producing hypoglycaemia. Diabetes Metab Rev. 1991. 7:79–91.
2. de Groot JW, Rikhof B, van Doorn J, Bilo HJ, Alleman MA, Honkoop AH, van der Graaf WT. Non-islet cell tumour-induced hypoglycaemia: a review of the literature including two new cases. Endocr Relat Cancer. 2007. 14:979–993.
3. Beckers MM, Slee PH, van Doorn J. Hypoglycaemia in a patient with a gastrointestinal stromal tumour. Clin Endocrinol (Oxf). 2003. 59:402–404.
4. Lee KW. Hypoglycemia. J Korean Soc Endocrinol. 1993. 8:231–240.
5. Service FJ, McMahon MM, O'Brien PC, Ballard DJ. Functioning insulinoma-incidence, recurrence, and long-term survival of patients: a 60-year study. Mayo Clin Proc. 1991. 66:711–719.
6. Miettinen M, Lasota J. Gastrointestinal stromal tumors (GISTs): definition, occurrence, pathology, differential diagnosis and molecular genetics. Pol J Pathol. 2003. 54:3–24.
7. Fletcher CD, Berman JJ, Corless C, Gorstein F, Lasota J, Longley BJ, Miettinen M, O'Leary TJ, Remotti H, Rubin BP, Shmookler B, Sobin LH, Weiss SW. Diagnosis of gastrointestinal stromal tumors: a consensus approach. Hum Pathol. 2002. 33:459–465.
8. Luo XL, Liu D, Yang JJ, Zheng MW, Zhang J, Zhou XD. Primary gastrointestinal stromal tumor of the liver: a case report. World J Gastroenterol. 2009. 15:3704–3707.
9. Pink D, Schoeler D, Lindner T, Thuss-Patience PC, Kretzschmar A, Knipp H, Vanhoefer U, Reichardt P. Severe hypoglycemia caused by paraneoplastic production of IGF-II in patients with advanced gastrointestinal stromal tumors: a report of two cases. J Clin Oncol. 2005. 23:6809–6811.
10. Davda R, Seddon BM. Mechanisms and management of non-islet cell tumour hypoglycaemia in gastrointestinal stromal tumour: case report and a review of published studies. Clin Oncol (R Coll Radiol). 2007. 19:265–268.
11. Rikhof B, Van Den Berg G, Van Der Graaf WT. Non-islet cell tumour hypoglycaemia in a patient with a gastrointestinal stromal tumour. Acta Oncol. 2005. 44:764–766.
12. Hamberg P, de Jong FA, Boonstra JG, van Doorn J, Verweij J, Sleijfer S. Non-islet-cell tumor induced hypoglycemia in patients with advanced gastrointestinal stromal tumor possibly worsened by imatinib. J Clin Oncol. 2006. 24:E30–E31.
13. Escobar GA, Robinson WA, Nydam TL, Heiple DC, Weiss GJ, Buckley L, Gonzalez R, McCarter MD. Severe paraneoplastic hypoglycemia in a patient with a gastrointestinal stromal tumor with an exon 9 mutation: a case report. BMC Cancer. 2007. 7:13.
14. Singh R, Grey A, Miller M, Gresnigt MG, Hoogerbrugge CM, van Doorn J. Non-hyperinsulinemic hypoglycemia in a patient with a gastrointestinal stromal tumor. Eur J Intern Med. 2006. 17:127–129.
15. Guiteau J, Fanucchi M, Folpe A, Staley CA 3rd, Kooby DA. Hypoglycemia in the setting of advanced gastrointestinal stromal tumor. Am Surg. 2006. 72:1225–1230.
16. Daughaday WH, Emanuele MA, Brooks MH, Barbato AL, Kapadia M, Rotwein P. Synthesis and secretion of insulin-like growth factor II by a leiomyosarcoma with associated hypoglycemia. N Engl J Med. 1988. 319:1434–1440.
17. Firth SM, Baxter RC. Cellular actions of the insulin-like growth factor binding proteins. Endocr Rev. 2002. 23:824–854.
18. Blay JY, Reichardt P. Advanced gastrointestinal stromal tumor in Europe: a review of updated treatment recommendations. Expert Rev Anticancer Ther. 2009. 9:831–838.
19. Blay JY, Bonvalot S, Casali P, Choi H, Debiec-Richter M, Dei Tos AP, Emile JF, Gronchi A, Hogendoorn PC, Joensuu H, Le Cesne A, McClure J, Maurel J, Nupponen N, Ray-Coquard I, Reichardt P, Sciot R, Stroobants S, van Glabbeke M, van Oosterom A, Demetri GD. GIST consensus meeting panelists. Consensus meeting for the management of gastrointestinal stromal tumors. Report of the GIST Consensus Conference of 20-21 March 2004, under the auspices of ESMO. Ann Oncol. 2005. 16:566–578.
20. Yoo IR. The role of 18F-fluorodoxyglucose positron emission tomography in gastrointestinal stromal tumors. Nucl Med Mol Imaging. 2008. 42:S46–S51.
 XML Download
XML Download