

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Depression affects 10% to 30% of the people with diabetes worldwide [1]. A recent survey indicated that, globally, individuals with diabetes had greater odds of experiencing an episode of depressive symptoms than those without diabetes [2]. Diabetes patients with depression are at increased risk for poor glycemic control and development of cardiovascular complications and have higher mortality rates [134]. One of the behavioral mechanisms that may link depression with poor outcomes in diabetes is suboptimal diabetes self-care behaviors. In developed countries, patients with comorbid depression and diabetes have been found to have less frequent fruit and vegetable intake, more frequent fat intake, more sedentary behaviors, and fewer exercise sessions per week [567]. Moreover, smoking was twice as prevalent among depressed than among non-depressed diabetes patients [4]. However, studies on the association between depression and self-care in diabetes patients are scarce in the Sub-Saharan African context. Nevertheless, studies that have looked at the association between depression and other chronic illnesses, especially human immunodeficiency virus (HIV) and acquired immune deficiency syndrome (AIDS), have consistently found that depression is associated with suboptimal self-care in patients [8910].
Diabetes care mostly consists of self-care behaviors [11]. After consultations with their health care providers, patients are responsible for their diabetes care 24 hours per day. Optimal outcomes in diabetes require diligent daily self-care [4]. Diabetes self-care comprises the proper use of medication (insulin or oral medication, correct timing, and correct doses), counting carbohydrates, maintaining a healthy diet (e.g., low in saturated fat, low in salt, high in vegetables and fruits, and moderate alcohol intake), being physically active, monitoring blood glucose levels, maintaining proper foot care, and refraining from smoking, among others [12].
Major depressive disorder is a medical illness that affects feelings, thoughts, and behaviors. Depression results from persistent feelings of sadness and loss of interest in previously enjoyed activities [1314].
Cross sectional as well as systematic review studies showed that baseline levels of depression symptoms significantly predicted medication non-adherence at follow-up [1516]. For an increase of one point on a baseline depression score, there was a 1.08-fold increase in the odds of non-adherence to medication at follow-up [15]. Similarly, Lin and colleagues [4] observed that on average, depressed patients did not adhere to oral hypoglycemic medication 80 days in the previous year, compared to 62 days for non-depressed patients. The average percentage of non-adherent days was 25% in depressed patients compared to 19% in non-depressed patients [4].
A recent study conducted among Dutch patients showed that, in particular, depressed mood, sleeping difficulties, appetite problems, and suicidal ideation were significantly related to higher glycosylated hemoglobin (HbA1c) in patients with type 1 or type 2 diabetes mellitus (T1DM/T2DM) [14]. Therefore, the aim of the present study is to explore the associations between depression symptoms and diabetes self-care in Zambian individuals with diabetes.
Go to : 
METHODS
Design
This study employed a cross-sectional design. We assessed the link between the independent variables of interest (e.g., diabetes self-care, type of diabetes, age, sex, socioeconomic status [SES], and body mass index [BMI]) and the dependent variable, depression [17].
Study sample
The study sample comprised outpatients with either T1DM or T2DM, whether on insulin or oral treatment, from major urban hospitals in Lusaka, Ndola, Kitwe, and Livingstone. The T1DM or T2DM diagnosis was based on what was indicated on the patients' hospital record cards and their verbal confirmation. Patients were invited to participate in the study if they were at least 12 years old and were diagnosed at least 6 months before the study. A total of 157 patients signed the informed consent form and were recruited over a period of 1 year. Assent was obtained from patients younger than 18 years old whose guardians had consented their participation in the study. Table 1 shows the demographic characteristics of the participants.
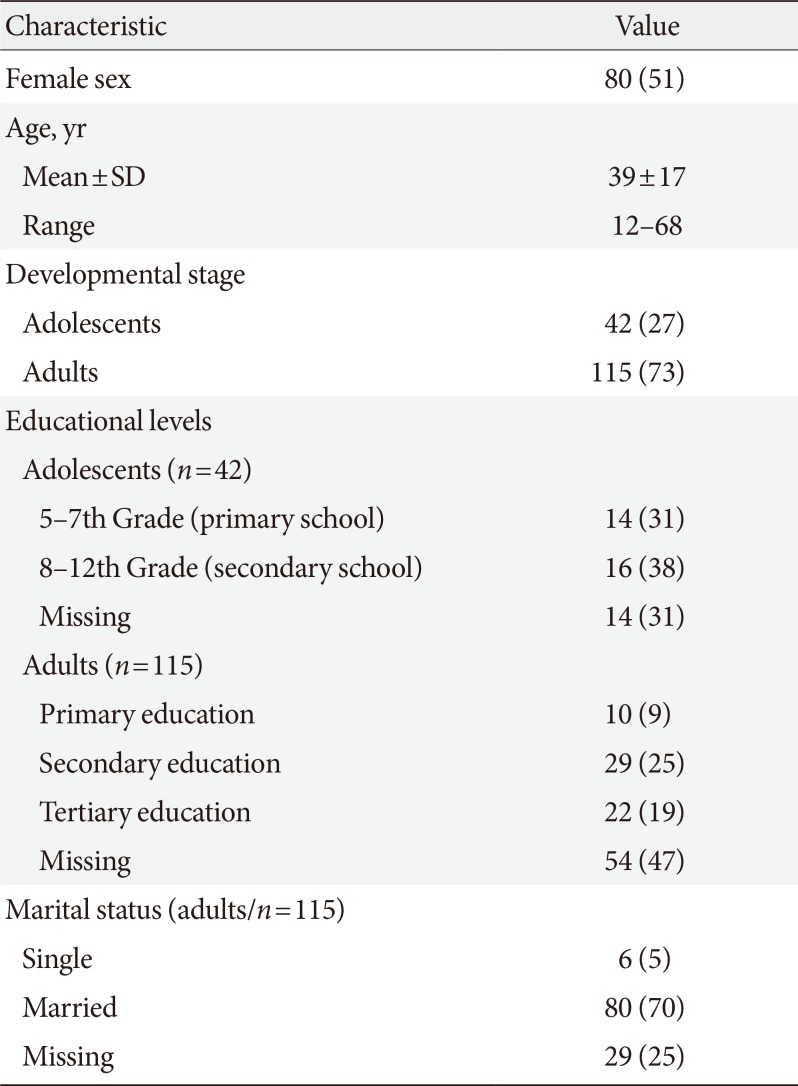
Table 1
Demographic characteristics of 157 participants (12 to 68 years) with type 1 and type 2 diabetes mellitus
![]()
Measures
Demographic variables
Information on age, sex, education level, asset index (properties and services owned by families of participants), and diabetes type were obtained.
Diabetes self-care
The 13-item diabetes self-care inventory (SCI) is a self-report measure used to assess patients' perceptions of their adherence to diabetes self-care recommendations over the past month [18]. Individuals rate themselves on a 5-point Likert scale that indicates how well they followed recommendations for self-care during the previous month (i.e., 1= “never do it” to 5= “always do this as recommended, without fail”) on several items, including glucose testing, administering the correct insulin dose, eating proper food, adhering to the meal plan, and exercising regularly. Individual items can be studied, and an overall adherence score is derived using the average of items 1, 2, 5, 7, 8, and 13; these items cover areas that are linked to better metabolic control [18]. The “wearing a medic alert ID” question was dropped because it did not apply to Zambian patients. Higher scores on the scale indicate good diabetes self-care. The SCI shows good reliability, with values of Cronbach's α of 0.84 for T1DM and 0.85 for T2DM [19]. In the current study, Cronbach's α was 0.71 and Lambda2 was 0.74.
Depression
We used the symptoms from the major depression inventory (MDI), a 12-item, self-report questionnaire used to assess depression [20]. Items of the MDI ask the patient to rate how long in the past 2 weeks each of the depressive symptoms was present on a six-point scale, ranging from 0 “not at all” to 5 “all the time.” Examples of items are, “Have you felt low in spirit or sad, have you felt less self-confident, have you suffered from reduced appetite?” and so on. The instrument can measure severity of depression with a score range from 0 to 50. According to the manual (based on Western norms), an MDI total score between 0 and 24 indicates “no depression to mild depression,” 25 to 29 “moderate depression,” and 30 to 50 “severe depression.” Items 8 and 10 are divided into two sub-items, (a) and (b). Only the highest scores of item 8 and 10 (either [a] or [b]) are included in the statistical analysis. This self-report measure contains 10 of the International Classification of Diseases, 10th edition (ICD-10) symptoms of depression and is identical to the Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV) symptoms apart from one that relates to low self-esteem [20]. Previous studies using the MDI showed higher values of Cronbach's α of 0.89 [21] and 0.94 [20]. In the current study, the value of Cronbach's α was 0.79 and the value of Lambda2 was 0.80.
Ethics approval and consent to participate
The study was approved by the Ethics Committee of the School of Humanities and Social Sciences, University of Zambia (reference number IRB, 00006464; IORG, 005376). The study only used data from participants that consented to participate in the study. Assent was obtained from participants younger than 18 years old.
Statistical analyses
Descriptive statistics on demographic characteristics were first conducted. We then conducted a t-test to examine types of diabetes and age group differences in self-care. Linear regression analysis was conducted between depressive symptoms as assessed by the MDI and diabetes self-care total score and individual items. Using a hierarchical approach, we adjusted our linear regression models for the following potentially confounding variables: sex, age, SES, type of diabetes, and BMI. P<0.05 was considered statistically significant. All analyses were conducted with SPSS version 16.0 (SPSS Inc., Chicago, IL, USA).
Go to :
RESULTS
Demographic data
Table 1 shows the demographic characteristics of the sample. Of the 157 participants, 80 were females (51%). Mean age was 39±17 years, with ages ranging from 12 to 68 years. Of the total sample, 115 (73%) were adults. About 25% of the adults had secondary education. About 69% of the adolescents were school-going, and the rest had not indicated their education level. Most of the adult subjects (80%) were married. Table 2 shows that a total of 93 subjects (59%) were classified as having T1DM in their medical charts, and 58 (37%) had T2DM. The type of diabetes for six patients could not be determined because the clinical record cards for these patients were not available at the time data was collected, but they had either T1DM or T2DM. In the total sample, the mean BMI was 25±5 kg/m2. The mean BMI was 22±4 kg/m2 for adolescents and 27±5 kg/m2 for adults. The BMI for males was 25±5 kg/m2 and for females 26±5 kg/m2.
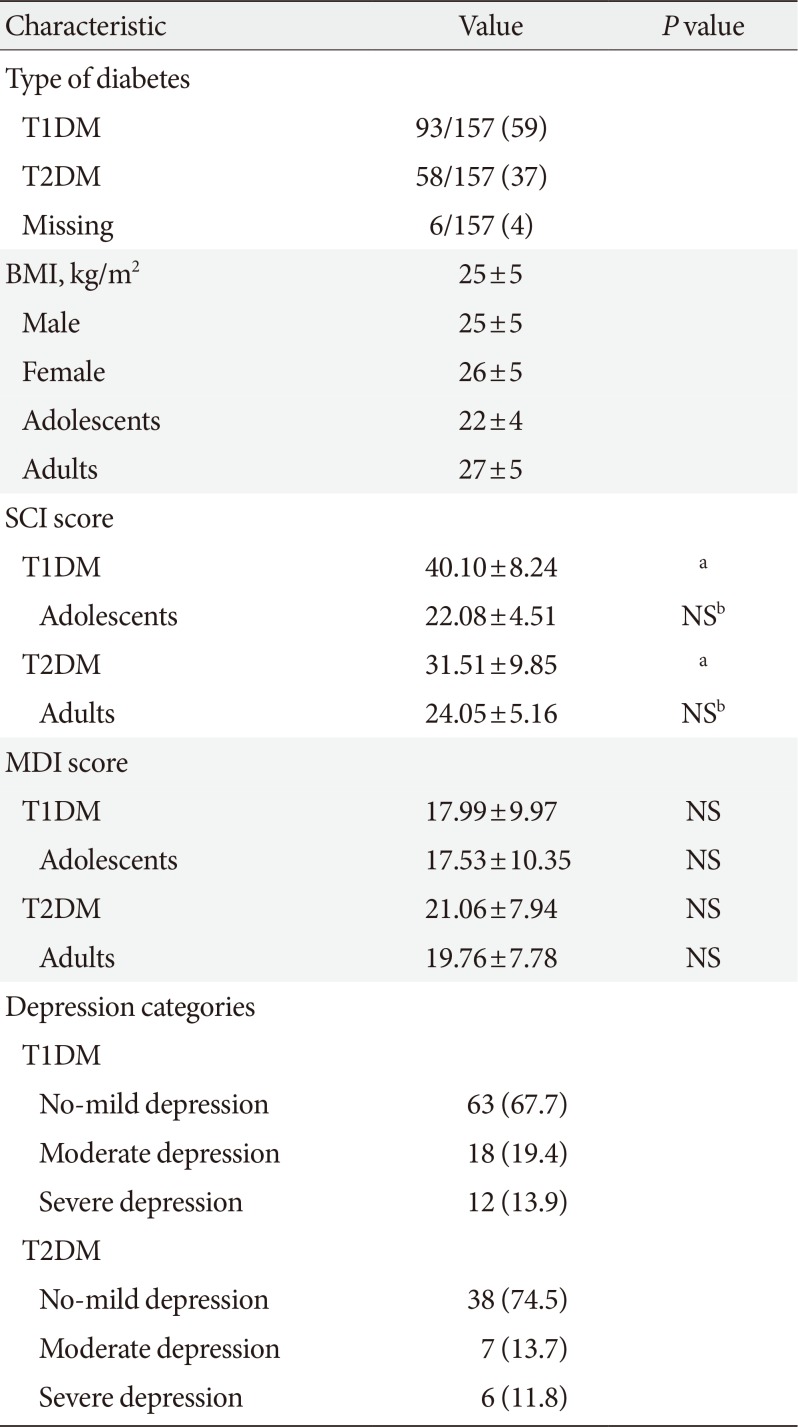
Table 2
Clinical characteristics of the participants (n=157)
![]()
Proportions of depression and self-care
Based on the cutoff of the measure, 13.8% of individuals with T1DM had severe depression, and 11.8% with T2DM had severe depression. Table 3 shows that the most reported symptom of depression in individuals with T1DM was increased appetite (39.8%), followed by feeling restless (29%), that life was not worth living (26.9%), and lack of energy and strength (25.8%). For individuals with T2DM, the most reported symptoms of depression were increased appetite (64%), feeling restless (32%), and reduced appetite (28.8%). Disaggregated data on age group differences showed that the most reported symptoms in adolescents were increased appetite (34.9%), bad conscience or feeling guilt (34.9%), and feeling a lack of energy (30.2%), whereas for adults they were increased appetite (50.9%), and feeling restless (31.6%). The mean depression score was 19.12±8.95, and there was no statistically significant difference between individuals with T1DM and T2DM on depression score (t=−1.74, df=118, P>0.05). However, there was a statistical difference between individuals with T1DM and T2DM on the self-care score, with T1DM patients showing higher scores (t=5.24, df=97, P<0.001). The majority of patients scored above the midpoint of the self-care scale (19.52±6.06). The majority of patients with T1DM reported ketone testing (67%), glucose recording (56%), and glucose testing (52%) as major problems related to self-care activities. For individuals with T2DM, the major problems were glucose testing (71%) and eating regular snacks (66%). For adolescents with diabetes, the major self-care problems were ketone testing (63%) and carrying quick-acting sugar to treat reactions (47%), whereas for adults, they were glucose recording (65%), ketone testing (65%), and glucose testing (64%). For detailed results, see Table 3.
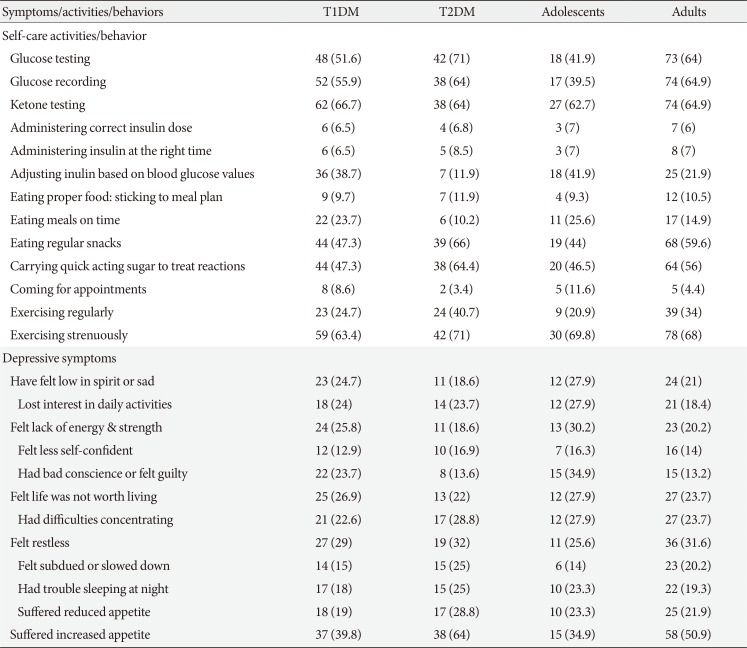
Table 3
Type of diabetes disaggregated proportions of below average self-care activities/behaviors and depressive symptoms
Values are presented as number (%). Below average (“never do it” and “sometimes follow recommendations”), average (“follow recommendations 50% of the time”), above average (“usually do as recommended; occasional lapses” and “do as recommended without fail”), better if below average.
T1DM, type 1 diabetes mellitus; T2DM, type 2 diabetes mellitus.
![]()
The association between depressive symptoms and diabetes self-care
Our results (Table 4) showed no association between depression symptoms and total diabetes self-care (β=0.10, P>0.05). This association remained nonsignificant even after controlling for demographic characteristics. We then conducted linear regression analyses to study the associations between the 13 diabetes self-care activities and the total score of depression while controlling for demographic characteristics. Linear regression analyses showed depression was associated with de-creased glucose testing (β=−0.27, P<0.05) and eating a meal on time (β=−0.23, P<0.05) (Table 5). Other self-care activities were not associated with depression. The controlled demographic characteristics that remained significant were that age (being young) was associated with poor diabetes self-care (β=−0.24, P<0.05) and BMI (β=0.33, P<0.01), and there was a borderline association between high SES and increased self-care (β=0.15, P<0.057). Having T2DM (β=−0.12, P>0.05) and being female (β=−0.03, P>0.05) were not associated with diabetes self-care.
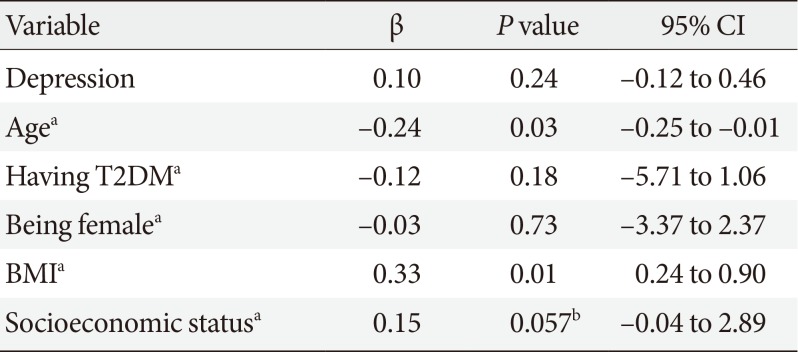
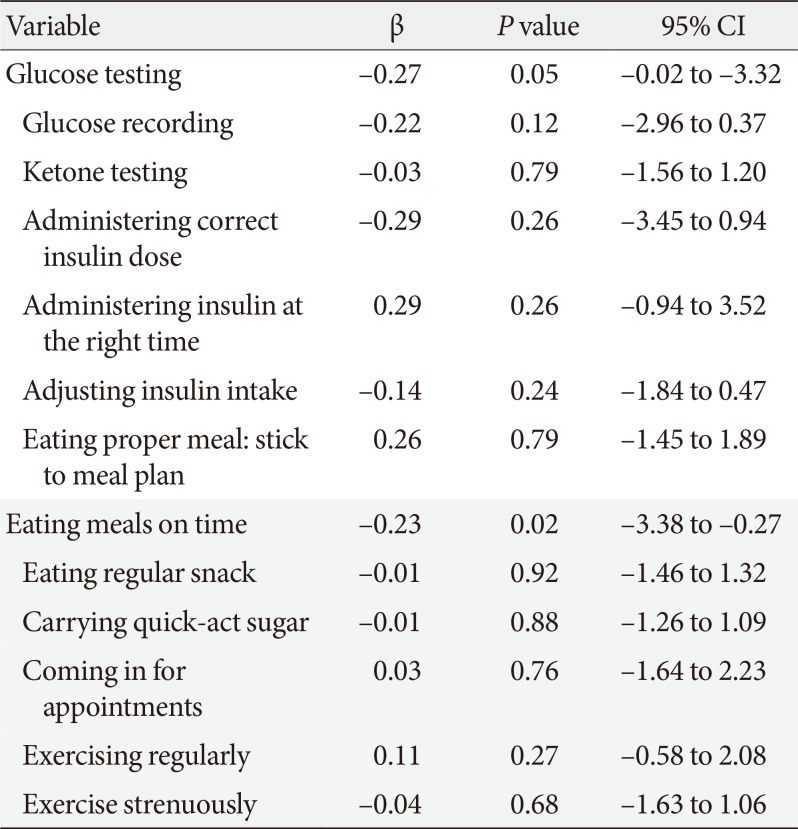
Table 4
The association between diabetes self-care, depression and demographic characteristics
![]()
Table 5
Standardized regression coefficient from linear regression analysis for the association between depression score and diabetes self-care activities (n=157)
![]()
Go to :
DISCUSSION
The aim of the present study was to explore the association between depression as measured by the MDI and diabetes self-care as measured by the SCI. Our first model showed that there was no association between depression total score and diabetes self-care total score. Diabetes self-care involves a number of activities, many of which are measured by the SCI. All of these behaviors or activities (proper use of medication such as insulin or oral medication; counting of carbohydrates; eating a healthy diet, e.g., low in saturated fat, low in salt, high in vegetables/fruits, and moderate alcohol intake; being physically active; and monitoring of blood glucose levels) are designed to improve glycemic control and reduce risk of developing complications caused by poorly managed diabetes [12]. Therefore, we decided to run a linear regression model assessing the association between depression and the 13 self-care activities measured by the SCI. Results showed that depression was associated with decreased glucose testing and not eating meals on time. Other activities were not significantly associated with depression. The most important objective of monitoring blood glucose level is the assessment of overall glycemic control and initiation of appropriate steps in a timely manner to achieve optimal control. In our sample, glucose testing was an important self-care activity that helps in glycemic control and was associated with depression. Moreover glucose testing was one of the highly self-reported problems (61%) among our sample. Self-monitoring of glycemic control is a cornerstone of diabetes care that can ensure patient participation in achieving and maintaining specific glycemic targets [1222]. Self-monitoring provides information about current glycemic status, allowing for assessment of therapy and guiding adjustments in diet, exercise, and medication to achieve optimal glycemic control. It was also not surprising that depression was associated with not eating meals on time. Eating meals on time helps reduce hypoglycemia. Hypoglycemia occurs when a person's blood sugar (glucose) level falls too low. These two self-care activities (glucose testing and eating a healthy diet on time) are necessary to help a physician and patient make adjustments of other self-care activities such as exercising, going for appointments, carrying quick-acting sugar to treat reactions, administering correct insulin, and adjusting insulin intake.
Although only two self-care activities were associated with depression, the majority of individuals in our study reported below average self-care activities on ketone testing (80%), glucose recording (62%), and glucose testing (60%), eating regular snacks (57%), and carrying quick-acting sugar to treat reaction (56%). This was not surprising because patients in Zambia can only test for ketone and sometimes glucose at the hospital because they cannot afford to have a glucometer of their own or to buy ketone strips. Most of the patients test their glucose at the hospital, so glucose recording is not possible for most of them at home. Their glucose monitoring history is only avail-able in their hospital record files. This is a challenge, given that most of the patients have a hospital appointment every 3 months (pediatric section) unless there is an emergency or they experience recurrent hypoglycemia or are requested to appear for an early appointment by a physician. A qualitative study among adolescents with T1DM in Zambia showed that most patients could not afford to have meals or even carry a snack or quick-acting sugar to treat reactions, “So we all have to come here for reviews and some come from very far and transport is very expensive. But also money for food is a problem. Especially if I am here and I am hungry I need money to buy food, I was told to be eating but I cannot get money here to buy food” [23].
Similar to other studies [24], we found that age, BMI, and to some extent, SES were associated with self-care. Being young was negatively associated with self-care. We speculate that being young was negatively associated with self-care because young people often experience conflicts of priorities that negatively affect their self-care behaviors. Young people often forget to adhere to their regimen because they engage in many competing activities, feel embarrassed in the presence of their peers, and are less inclined to engage in self-care behaviors compared to adults. These results must be interpreted with caution because other studies suggest that older people have elevated depression, which may interfere with their diabetes self-care behaviors compared to young people [25]. Increase in BMI was associated with poor self-care. Similar results were found in Australia among 1,796 respondents with T2DM when a group with BMI ≥35 kg/m2 was found to be less likely to achieve healthy diet and exercise targets and placed less importance on diet and exercise recommendations [26]. An increase in BMI is associated with low self-esteem, which may also affect self-care activities. BMI is particularly documented to predict poor glycemic control [27]. Although females are more likely to be depressed than men [228], we did not find any association between sex of the participants and self-care activities. We also found that high SES was positively associated with self-care. Although SES is a proxy for a wide variety of factors, these results could suggest that individuals with high SES have readily available money to buy healthy food and required medication and engage in social activities that do not side-track them from self-care activities compared to patients with low SES.
The strength of the present study is that it used the MDI, which is based on the DSM-IV, ICD-10 symptoms of major depression, and the SCI, which covers all recommended critical areas of diabetes self-care [1826]. Limitations of the study are that we do not know the refusal rate, so there might have been a selection bias, although it is difficult to estimate how big this selection bias was. The sample size was small due to recruitment difficulties also; as a consequence, probability sampling could not be used. In addition, we were unable to screen for other illnesses, such as HIV, and assess the effects of different treatment modalities and biochemical markers such as HbA1c, which could have a confounding effect on our results. Finally, we cannot rule out a possible overestimation of self-care activities and underestimation of depressive episodes by our respondents due to social desirability often found in self-report measures. Moreover, the SCI and the MDI have no norms; also, the former was not validated for the Zambian sample. However, in its form, the SCI had items that tapped into common self-care activities except for one that was dropped, “wearing a medic alert ID,” because no subjects who participated in the study had one. This measure can be made more robust by adding items such as “receiving reminders from family/friends to take medication” and “accessing medical essentials, e.g., syringes.”
Depression is associated with less frequent glucose testing and lack of adherence to meal plans by patients with diabetes. Some variance in poor self-care is explained by demographic characteristics, specifically, age, BMI, and to some extent SES. Therefore, clinicians need to screen and treat individual depressive symptoms in patients with diabetes, especially among young people, patients with low SES, and those with high BMI. Given the lack of manpower in cognitive behavioral therapy in Zambian hospitals, we, in the meantime, recommend the use of anti-depressants in treating depression; these have not only been found to be effective in treating depression [293031], but are free and readily available in Zambian major hospitals. Specifically, if drugs are to be prescribed, we recommend the use of selective serotonin reuptake inhibitors, which has been found to be associated with improved glycemic control [32]. Not only is depression management meaningful from the perspective of a patient's quality of life, it may also have beneficial implications for patients' ability to achieve and maintain diabetes self-care goals [29]. In addition to depression treatment, patients with diabetes ought to be helped to optimize self-care by enhancing self-efficacy, healthy eating, physical activities, monitoring of blood sugar, good problem-solving skills, healthy coping skills, risk-reduction behaviors, and compliance with medication instructions [12]. Therefore, interventions should simultaneously address depression symptoms and self-care skills to achieve optimal diabetes outcomes.
Go to :
 XML Download
XML Download