

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Diabetes mellitus (DM) is well known for its chronic course, with debilitating complications that require long-term management and treatment. A bidirectional relationship between depression and DM has been frequently reported [1], with ever increasing health costs as a notable adverse consequence [2]. A negative impact of depression on patients with DM has been reported from several perspectives. Depressive symptoms were closely associated with higher readmission and mortality rates [3], and a link between renal complications with diabetes was discussed in a recent study [4]. In addition, an 11-year follow-up revealed that the risk of diabetic foot ulcers increased in DM patients with depression [5].
Regarding the association between depression and DM, the influence that depression has on mortality rates warrants special clinical attention to discover predictors of mortality in DM patients, which could be conducive to setting up a proper paradigm to manage and treat DM patients systematically. Indeed, the importance of accurate depression screening in DM patients has been repeatedly emphasized [6]. Moreover, antidepressant drug prescription for depressed DM patients remarkably increased the effectiveness of glycemic control [7], and a need for further evidence-based lifestyle interventions has been suggested through a recent systematic review [8].
Recent studies have actively demonstrated a close relationship between depression and mortality rates in DM patients. Depressive symptoms proportionally increased mortality rates in type 2 diabetes mellitus (T2DM) patients who were not treated with insulin in one study [9], and a two-fold increase in mortality rates in T2DM patients with anhedonia was reported in another study [10]. In addition, the illness duration of depression significantly predicted mortality rates in a dose-dependent manner in one elderly cohort [11]. Despite the relatively large cohorts recruited in the aforementioned studies, most of them adopted depression scales to evaluate the relationship between depression and DM. Therefore, it is not clear whether their cohorts were patients who had been actually diagnosed with depression.
To summarize briefly the local data from Korea regarding depression and DM, the prevalence of depression in T2DM patients has been reported to be as high as 28.8% [12]. One national study sample on Korean women reported a prevalence of 22.6% in DM patients reporting symptoms of depression [13]. Risk factors for depression were reported, including oral diabetes medicine or insulin, low-incomes, smoking, and lack of exercise [12]. Despite such data available for the Korean sample, reports on the mortality rates in Korean DM patients comorbid with depression are relatively scarce despite its clinical importance.
In this study, patients with a dual diagnosis of DM and depression according to clinical interviews following the International Classification of Disease, 10th revision (ICD-10) were included to increase objectivity. Moreover, it is one of the few studies to report on the link between mortality rates and depressed DM patients in the Korean population. We hypothesized that DM patients with depression would demonstrate higher mortality risk than those without depression.
Go to : 
METHODS
Source of database
The National Health Information database maintained by the Korean National Health Insurance Service (NHIS) was used. Retrospective data from January 2003 to December 2013 were collected for adult T2DM patients older than 30 years. The database includes specific information on the demographic characteristics, consultation statements, and diagnosis by the ICD-10 and prescription. Large-scale studies using the NHIS database have been conducted previously [14], and these data are widely accepted to be representative of the entire Korean population, which increases its utility as a source of data for population-based nationwide studies. This study was approved by the Institutional Review Board of the Korean National Institute for Bioethics Policy (P01-201504-21-005), through which informed consent was exempted.
Definition of diabetes mellitus, depression, and death
All participants were diagnosed with T2DM according to ICD-10 codes at baseline, and patients over the age of 30 years with a diagnostic code (ICD-10) of T2DM (E11-E14) more than once in a given year from January 2003 to December 2013 were included. They all made at least one visit to outpatient care or inpatient care to diagnose T2DM and accepted at least one prescription of antidiabetic medication, excluding prediabetes and non-diabetes subjects. Antidiabetic drugs included seven classes of medications dispensed during the study period in Korea (i.e., biguanide, sulfonylurea, α-glucosidase inhibitor, dipeptidyl peptidase-4 inhibitors, thiazolidinedione, meglitinide, and insulin). The glucagon-like peptide-1 agonist, with its relatively recent introduction in 2008 and subsequent insurance coverage in 2010, was not included. We defined the depressed T2DM group diagnosed with both T2DM and depression (F320-F349) according to the ICD-10 codes at baseline. In addition, patients with at least one prescription for antidepressants were also included. Claims data and national mortality data from the National Statistical Office to define death were merged for the analysis.
Statistical analysis
The demographic characteristics and the mortality rates for the participants were analyzed through descriptive statistics. The annual prevalence of depression was estimated according to the T2DM diagnosis status, and the age groups were stratified into five groups (30 to 39, 40 to 49, 50 to 59, 60 to 69, 70 to 79, and ≥80). Mortality rates and hazard ratios for each age group of those diagnosed with T2DM in 2003 were estimated using a Cox proportional hazard method with the Kaplan-Meier cumulative survival curve showing overall survival rates according to T2DM status, until the given year of 2013.
Go to :
RESULTS
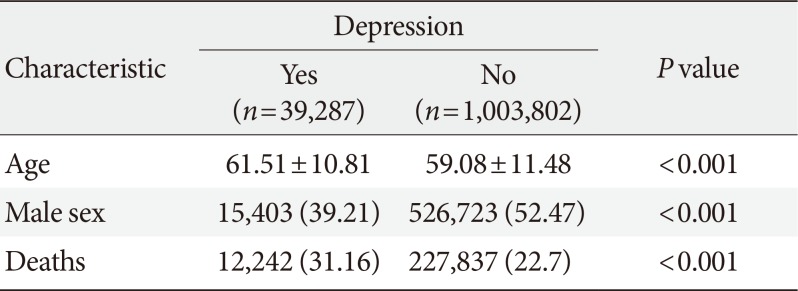
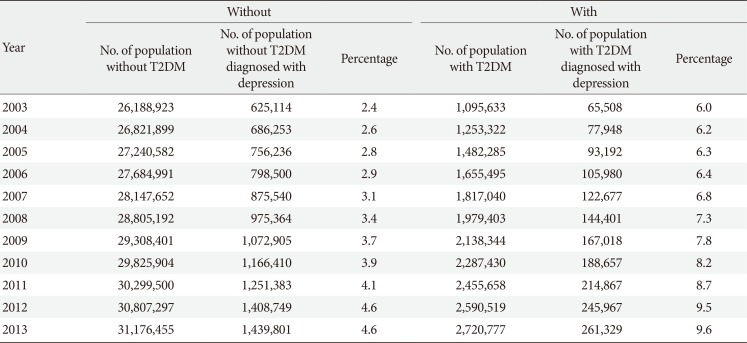
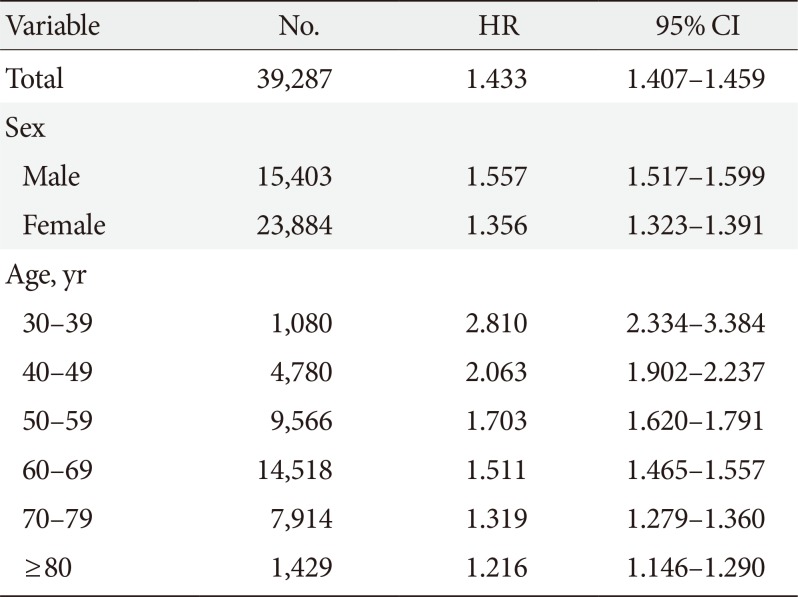
The demographic characteristics of patients with T2DM at baseline in 2003 are illustrated in Table 1. Comparisons of the annual prevalence of depression between the population with and without T2DM diagnosis from 2003 to 2013 demonstrated that, the annual prevalence of depression was consistently higher in the T2DM group (Table 2). Moreover, the annual prevalence of depression increased in both groups during the period of observation. Compared to 2003, the prevalence rates for depression in both groups increased by nearly two-fold in 2013. The unadjusted Cox model mortality hazard ratio for the T2DM group with depression was 1.43 when compared to those without depression (Table 3). The Kaplan-Meier cumulative survival curve is illustrated, with the non-depressed group showing a higher survival probability (Fig. 1). The mortality hazard ratio increased further in the male group, and the highest mortality hazard ratio was noted in the age group of 30 to 39, with the ratio decreasing proportionally in subsequent, older age groups (Table 3).
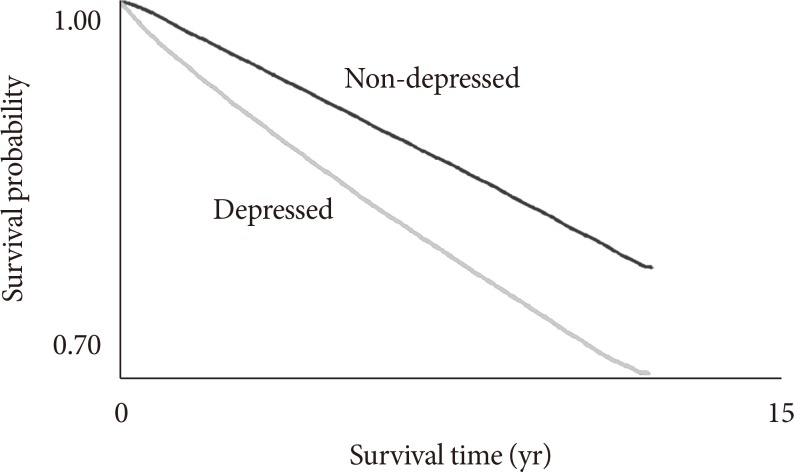 | Fig. 1Survival curves for two groups: type 2 diabetes mellitus (T2DM) with depression and T2DM without depression.
|
Table 1
Demographic characteristics and mortality rates of type 2 diabetes mellitus patients with and without depression, Korea at baseline (2003)
| Characteristic | Depression | P value | |
|---|---|---|---|
| Yes (n=39,287) | No (n=1,003,802) | ||
| Age | 61.51±10.81 | 59.08±11.48 | <0.001 |
| Male sex | 15,403 (39.21) | 526,723 (52.47) | <0.001 |
| Deaths | 12,242 (31.16) | 227,837 (22.7) | <0.001 |
![]()
Table 2
Comparisons of annual prevalence rates of depression in between population with T2DM and without T2DM from 2003 to 2013 in Korea
![]()
Table 3
Mortality hazard ratio of type 2 diabetes mellitus patients with depression diagnosed in 2003
![]()
Go to :
DISCUSSION
To the best of our knowledge, this is the first Korean population-based study to delineate the association of depression and mortality in T2DM patients. Our results indicate that T2DM patients with depression exhibited a significantly higher mortality risk than those without depression. In particular, the mortality risk increased in the male group and younger age groups. We believe that the aforementioned association harbors several notable clinical implications.
First, the annual increase in prevalence of depression in T2DM patients between 2003 and 2013 is clinically meaningful. Despite that the annual prevalence of depression is ever increasing regardless of medical or psychiatric comorbidities, the increased prevalence of depression in this specific group of patients with T2DM patients warrants special attention. The reasons for such increases could be explored to expand awareness of the importance of early detection of depression and lessening the societal stigma for mental disorders. One recent study conducted door-to-door household surveys and noted this phenomenon, with an increased prevalence of major depressive disorders since 2001 [15]. Indeed, an underreporting of psychiatric symptoms has hampered an accurate estimation of the prevalence of mental disorders in Korea [15]. The same could have influenced the process of estimating the prevalence of depression in T2DM patients. Previous literatures have demonstrated a close link between DM and depression. To date, specific mechanisms involved in the bidirectional relationship between depression and DM, and their effects on mortality, remain elusive. An association between poor glycemic control and depression was previously reported [16], and a significant relationship between depression and diabetic complications was also demonstrated [17]. One study reported that amongst diabetic complications, diabetic neuropathic pain was a determinant for depression, suggesting pain management as an integral issue in diabetic care [18]. A previous Korean study demonstrated that DM patients were at high risk of depression and suicidal attempts, suggesting the detrimental effects of depression on the development of DM, with possible causative factors presumed to be increased physical inactivity and caloric intake [19]. Moreover, immunological dysfunction induced by depression in the trajectory of illness was purported to be a major culprit for mortality in another study [20].
Second, the increased mortality in T2DM patients with depression conveys an important message to clinicians. Increased mortality in T2DM patients in our results could be attributed to the aforementioned adverse effects of depression on DM. Regarding a specific relationship between mortality and DM, a recent meta-analysis of prospective studies on mortality in diabetic patients indicated that self-reported depressive symptoms were associated with all-cause mortality risk, with a hazard ratio of 2.56, and a meta-analysis on six studies based on depression diagnosis through clinical interviews revealed the adjusted hazard ratio to be 1.49 for depressed diabetic patients [21]. Another meta-analytic study on the mortality risk of depression in diabetic patients reported similar numbers, with a hazard ratio of 1.50 for the depressed diabetic individuals [22]. Although the heterogeneity between studies should be kept in mind with caution before interpreting results from meta-analytic studies, our results are somewhat consistent with the aforementioned reports, with a hazard ratio of 1.44 for the depressed T2DM group.
Third, a higher mortality risk was noted in the depressed male group in our results. Disparate mechanisms are involved during the illness, and surely, gender differences in vulnerability to depression, with well-known female preponderance, might affect mortality risk. In this regard, depressed women, but not men, were vulnerable to DM in one recent study [23]. However, our results differed from the aforementioned reports, with the depressed male diabetic group showing a higher mortality risk. One recent study suggested that in male T2DM patients, physical inactivity was associated with severe distress, and current smoking was more likely to distress male patients than female patients [24]. In an epidemiological study on depression in the Korean general population, a lack of libido was found to be the most prominent depressive symptom in the male population [25]. In line with this stance, a recent study found that T2DM was closely associated with sexual dysfunction, and more significantly, clinical depression was closely linked to erectile dysfunction in male T2DM patients [2627]. Moreover, a recent study on male T2DM patients indicated that proper therapeutic management with phosphodiesterase-5 inhibitors significantly ameliorated sexual dysfunction and depressive symptoms [28]. Thus, a more focused clinical management of sexual dysfunction is necessary in T2DM male patients who present depression.
The statistical results indicate a higher mortality risk in younger, depressed age groups, with the highest mortality risk in the youngest age group of the participants (aged 30 to 39). Two interpretations could explain this result. First, considering that the participants were all T2DM patients, it is less likely that the mortality of our depressed, younger groups reflect deaths from medical conditions. With regard to their older counterparts, medical conditions related to DM complications rather than depression itself could have influenced their mortality. Previous reports indicated that suicidal thoughts were less frequent in older age groups, with decreased frequency of reported symptoms of depression and anxiety at ages over 55 [29]. This phenomenon could have been reflected in our participants as well. Second, a study on the association between illness perception and depression in T2DM patients [30] revealed that the possible vulnerability of younger age groups can be extrapolated. T2DM, an illness with chronic course and complications, could be more devastating to younger age groups with more years of life expectancy than their older counterparts. More active psychological intervention in the younger age group diagnosed with T2DM patients is thus needed.
This study has several limitations that must be considered. First, because the mortality hazard ratios shown in the results were all unadjusted for other well-known risk factors, such as smoking status, alcohol consumption, body mass index, hypertension, cancer, cerebrovascular disease history, and diabetes complications, mortality from the aforementioned confounding factors cannot be excluded. However, we believe that the effect of depression in the overall mortality rates in T2DM patients still has strength, warranting special attention to those who present depressive symptoms during their illness. Second, because this epidemiological study is limited to the Korean population, it is difficult to generalize our results. Third, the selection criteria adopted to diagnose depression in the study was implemented using the code-based national registry; hence, a lack of structured interviews and scaled ratings by psychiatrists limits the accuracy of the association between depression and mortality in T2DM patients. Fourth, because all our participants were T2DM patients, further research is needed to elucidate the link between mortality and depression in type 1 DM patients. Fifth, because the causes of death of the participants were not clear, further research should be directed toward explicating the relationship between cause-specific mortality and depression.
Depression in T2DM patients significantly increased mortality risk, and more systematic interventions should be implemented to identify risk factors of depression and help those who need treatment for depression. Diabetes care should not be limited to resolving physical distress, but should be expanded to include systems enabling lifelong surveillance of patients' lifestyles, psychological health, and well-being.
Go to :
 XML Download
XML Download