

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Prediabetes is a high-risk state for diabetes that is typically defined as blood glucose concentrations higher than normal, but lowers than diabetes thresholds. Prevalence of prediabetes is increasing worldwide and more than 470 million people will have prediabetes by 2030 [1]. Around 5% to 10% of people with prediabetes become diabetic every year, with the same proportion converting back to normoglycaemia, although the conversion rate varies with population characteristics and prediabetes definitions [2].
Prolactin is a 23 kDa protein produced by the anterior pituitary gland in response to physiologic stress, sleep, pregnancy, nipple stimulation, and nursing; it is important for mammary gland development and differentiation during pregnancy and crucial for lactation and maternal behavior immediately after labor [3]. In addition to being a circulating hormone of pituitary origin, prolactin in humans is produced by non-pituitary sites including the endometrium, decidua, lymphocytes, brain, breast, and prostate, where it acts as a cytokine [4]. Besides its well-known lactogenic properties, prolactin is also a highly versatile hormone whose functions are related to reproduction, growth and development, metabolism, immune regulation, brain function, and behavior [56]. Maternal prolactin increases concurrently to insulin during the second half pregnancy and stimulates β-cell proliferation, insulin production, and insulin secretion [7]. Moreover, it has been found that the effect of prolactin on glucose metabolism is not confined to the period of pregnancy [68]. In a large community based study, high circulating prolactin was associated with lower prevalence of diabetes and impaired glucose regulation in middle-aged and elderly Chinese men and postmenopausal women [9].
Indeed, an inverse association of prolactin with cardiac remodeling was also previously suggested [10]. Cardiac remodeling referred to dynamic, incremental alterations in structure and function over the life course in the human heart [11]. The morphology of this progressive cardiac remodeling may be characterized by changes in multiple measurable echocardiographic indices including increased left ventricular mass (LVM), progressive left ventricular (LV) wall thickening, and a large spectrum of geometrical LV adaptations. These changes were associated with greater cardiovascular morbidity and mortality [12].
Therefore, the first question arises whether low serum prolactin is associated with adverse cardiac remodeling in subjects with prediabetes and if so what the impact of gender is? Second, could serum prolactin be considered a predictor of cardiac morbidity in those subjects? This study was conducted to assess serum prolactin level variations in relation to echocardiographic indices of cardiac remodeling; LVM and incident left ventricular hypertrophy (LVH); among adult men and women with prediabetes.
METHODS
This cross sectional study comprised 80 adults with prediabetes, 40 men and 40 premenopausal women, with a mean age of 45.31±4.47 years. Subjects with prediabetes were recruited from the Endocrinology and Obesity Outpatient Clinics at Mansoura Specialized Medical Hospital, Mansoura University, Egypt between February 2014 and January 2015. All subjects signed an informed consent and the study was approved by the Local Ethics Committee.
All study participants were subjected to a detailed medical history; data on physical activity were collected and participants underwent a clinical examination. Anthropometric measurements were obtained using standardized techniques; height was measured to the nearest 0.5 cm, body weight was measured to the nearest 0.1 kg, body mass index (BMI) was calculated as weight/height2 (kg/m2) and waist circumference (WC) was measured at the highest point of the iliac crest. Blood pressure was taken in the sitting position after 10 minutes of rest using a random-zero sphygmomanometer. Prediabetes was defined based on World Health Organization criteria [13]; people are at high risk of developing diabetes if they have one of two distinct states: impaired fasting glucose defined as a fasting plasma glucose (FPG) concentration of ≥6.1 and <7.0 mmol/L, without impaired glucose tolerance (IGT), and IGT defined as a FPG concentration of <7.0 mmol/L and a 2-hour postload plasma glucose (PPG) concentration of ≥7.8 and <11.1 mmol/L, measured during a 75 g oral glucose tolerance test.
Exclusion criteria were diabetes, hypertension or the use of antihypertensive medications, aortic stenosis, prevalent or incident myocardial infarction, history of pituitary disease, thyroid disorders, hepatic or renal failure, infection, connective tissue disorders, malignancy, pregnancy, women taking birth control pills or hormone replacement therapy and smoking. We also excluded six subjects with prolactin levels exceeding normal values for our laboratory (>23.3 ng/mL for women and 15.2 ng/mL for men) and those who were taking drugs known to influence glucose and prolactin, i.e., metformin, thiazolidinediones, steroids, metoclopramide, cimetidine, or psychoanaleptics.
Laboratory assay
FPG and 2-hour PPG were assayed using commercially available kit, Cobas (Integra-400) supplied by Roche Diagnostics (Mannheim, Germany). Glycosylated hemoglobin (HbA1c) was measured as an index of metabolic control on a DCA 2000 analyzer, fast ion exchange resin (Roche Diagnostic). The reference range was 4.4% to 6.4%. Fasting serum insulin was assayed by a solid-phase, enzyme-labeled chemiluminescent immunometric assay using an immulite analyzer supplied by Siemens (DPC Cirrus inc., Los Angeles, CA, USA). Homeostasis model assessment of insulin resistance (HOMA-IR) was calculated with the formula: HOMA-IR=[fasting insulin (µU/mL)×fasting glucose (mmol/L)/22.5] [14]. Total cholesterol, triglycerides, and high density lipoprotein cholesterol (HDL-C) were estimated by commercially available kits (Cobas Integra-400). Low density lipoprotein cholesterol was calculated according to Friedewald et al. [15]. White blood cells (WBCs) count was measured using Sysmex xs-500i (Sysmex Europe GmbH, Norderstedt, Germany; www.sysmex.europe.com/ifu). Prolactin levels were measured from frozen sera at −20℃ using electro chemiluminescent microparticle assay by Elecsys 2010 (Roche diagnostics; www.Roche.com); blood samples were drawn from the cubital vein in the supine position at morning after a minimum of 2-hour awaking time and 30 minutes of rest.
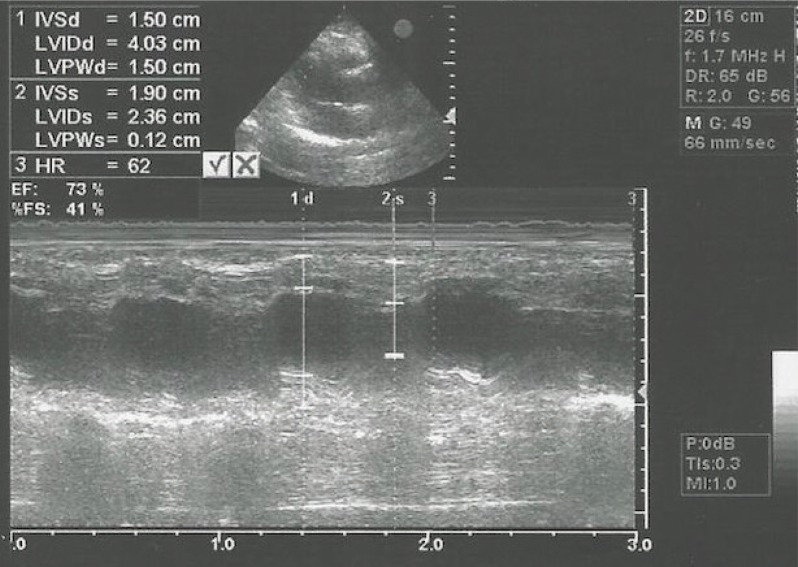
Two-dimensional and M-mode echocardiography was performed by certified physicians using a GE Vingmed vivid 3 ultrasound (GE Healthcare, Chicago, IL, USA). All data and measurements were stored digitally. LV dimensions (interventricular septum thickness [IVS], left ventricular posterior wall thickness [LVPWD], left ventricular diastolic dysfunction [LVDD], and left ventricular end-systolic dimension [LVDS]) were measured. LVM was calculated according to the following formula: LVM={0.80×[1.04×(LVDD+IVS+LVPWD)3−LVDD3]}+0.60/height2.7 [16]. LVH was defined by a LVM >48 g/m2.7 in men and >44 g/m2.7 in women (Fig. 1) [16].
Statistical methods
Data entry and analysis were done using the SPSS version 17 (SPSS Inc., Chicago, IL, USA). The data were expressed as mean±standard deviation for normally distributed data, frequency and proportion for categorical data and median (minimum–maximum) for skewed data. Statistical comparison between two groups was assessed by Student t-test for parametric data and Mann-Whitney for nonparametric data. A chi-square test was performed to compare categorical data. Univariate analysis was performed with LVM as the dependent variable and other studied variables as the independent. Univariate analysis was also performed with prolactin as the dependent variable and other studied variables as the independent (significant variables were entered in the regression model as co-founders); association between serum prolactin and LVM was performed by linear regression analysis with adjustment of the cofounding variables (age, WC, 2-hour PPG, HbA1c, HOMA-IR, HDL-C, WBC) in multivariable models. Moderation analysis was done to clarify the effect of sex on association between prolactin and LVM by determination of change in R2 significance between the two models; predictors in crude basal model were prolactin (is not centered) and sex (coded 1 for men and 0 for women), predictors in crude interaction model were prolactin, sex, and interaction between prolactin and sex. Moderation analysis was repeated after adjustment of the confounding variables affecting LVM. Logistic regression analysis was carried out to evaluate the association between prolactin and LVH prevalence in men and women with prediabetes with adjustment of the confounding variables in multivariate models. P≤0.05 was considered to be significant.
RESULTS
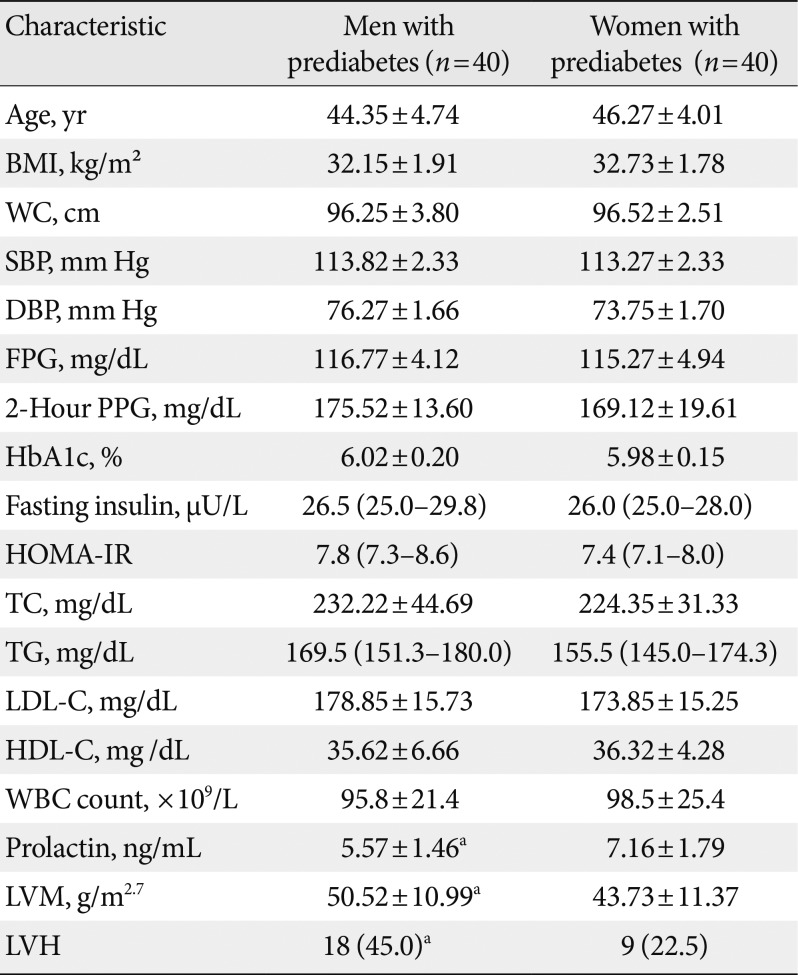
Table 1 presents the baseline characteristics of the study subjects stratified by sex. Prolactin was significantly lower in men than in women with prediabetes (5.57±1.46 vs. 7.16±1.79, P=0.008). LVM was significantly higher in men than in women with prediabetes (50.52±10.99 g/m2.7 vs. 43.73±11.37 g/m2.7, P=0.004). The proportion of LVH in men with prediabetes was 45% (18/40) compared with 22.5% (9/40) in women (P=0.03). No significant differences between men and women with regard to BMI, WC, blood pressure, plasma glucose, HbA1c, HOMA-IR, lipid profile, or WBC count.
With univariate analysis, LVM was significantly associated with age (B=0.69, P=0.01), WC (B=1.64, P>0.001), 2-hour PPG (B=0.02, P=0.01), HbA1c (B=21.53, P=0.003), HOMA-IR (B=4.86, P=0.01), HDL-C (B=−0.52, P=0.02), and WBC count (B=−0.52, P=0.02), whereas prolactin was significantly associated with WC (B=−0.04, P=0.03), 2-hour PPG (B=−0.08, P=0.008), HbA1c (B=−5.45, P=0.02), insulin (B=−0.41, P=0.03), HOMA-IR (B=−1.18, P=0.001), and WBC count (B=−3.91, P=0.001) (Supplementary Table 1).
We found a significant negative association between prolactin and LVM in men with prediabetes even after adjustment of other cofounding variables (age, WC, 2-hour PPG, HbA1c, HOMA-IR, HDL-C, and WBC) (B=−3.71; 95% confidence interval [CI], −5.86 to −1.56; P=0.001 in crude model; B=−2.46; 95% CI, −4.51 to −0.41; P=0.02 in adjusted model), whereas there was no significant association between prolactin and LVM in women (Table 2). The strength of the negative association between prolactin and LVM was significantly higher in men with prediabetes than in women (P values of R2 changes were 0.02 and 0.03 in crude and adjusted models, respectively) (Supplementary Table 2).
Furthermore, multiple logistic regression analysis was revealed a significant negative association between prolactin and prevalence of LVH in men with prediabetes after adjustment of confounding variables (odds ratio [OR], 0.39; 95% CI, 0.20 to 0.75; P=0.005 in crude model; OR, 0.39; 95% CI, 0.18 to 0.84; P=0.01 in adjusted model), whereas there was no significant association between prolactin and LVH in women (Table 3).
DISCUSSION
In the present study, men with prediabetes had significantly lower serum prolactin than did women. Our results also showed significant negative associations between prolactin levels and 2-hour PPG and HbA1c. These results are in harmony with Balbach et al. [17] who found an inverse association between prolactin and type 2 diabetes mellitus (T2DM) risk in a large population based cross-sectional study. Conversely, Wang et al. [9] found that a physiologically high circulating prolactin levels were associated with a favorable glucose metabolic profile; lower levels of FPG, PPG, and HbA1c; in a large community based middle-aged and elderly men and postmenopausal women.
Prediabetes is associated with the simultaneous presence of insulin resistance and β-cell dysfunction; abnormalities that start before glucose changes are detectable [1]. In the current study, HOMA-IR was significantly high in men and women with prediabetes according to normal limit for HOMA-IR <2.87, moreover the low prolactin levels were significantly associated with fasting insulin and HOMA-IR. In agreement, Wang et al. [9] observed that serum prolactin associates with higher levels of HOMA-β; however, a strict linear relationship was not confirmed across prolactin quartiles. Although some studies support the view that prolactin promotes insulin secretion [1819], other studies were not able to detect any correlation between prolactin and HOMA-IR [2021]. However, the role of prolactin on glucose metabolism and insulin resistance depends on its circulating concentration. It is worth mentioning that the effect of a physiologically high prolactin levels and pathological hyperprolactinemia on glucose metabolism could be different; excessive high levels of prolactin exacerbate whole-body and hepatic insulin resistance and impair the insulin secretory capacity in patients with hyperprolactinemia caused by prolactinoma [20].
From a mechanistic perspective, prolactin takes a crucial part in regulating whole-body insulin sensitivity and glucose metabolism by increasing β-cell proliferation, promoting cumulative insulin secretion, and inhibiting key caspases of the extrinsic and intrinsic pathways leading to islets apoptosis, and modulating immune function [8222324]. Prolactin up-regulates β-cell glucose uptake and utilization, whereas glucose increases islet prolactin receptor expression and potentiates the effects of prolactin on cell cycle gene expression and DNA synthesis [25]. Physiologically elevated prolactin levels also improve hepatic insulin sensitivity [26] and have an indirect action by increasing hypothalamic dopamine synthesis leading to improvement of energy and glucose homeostasis [2627].
Interestingly, recent studies revealed that human adipose tissue produces prolactin and also expresses prolactin receptors. Prolactin directly regulates adipose tissue function in down regulating lipoprotein lipase and fatty acid synthase [2829], which consequently suppress lipogenesis. On the other hand, insulin inhibits prolactin expression and release from differentiated adipocytes, so the overall effect of insulin on prolactin is likely inhibitory [30]. Collectively, these results raise the prospect that prolactin levels affect energy homeostasis through its action as an adipokine and is involved in the manifestation of insulin resistance [31].
We demonstrated that LVM and LVH were significantly higher in men than in women with prediabetes. With univariate analysis, LVM was significantly associated with WC, 2-hour PPG, HbA1c, HOMA-IR, HDL-C, and WBC count. We also found inverse independent associations of serum prolactin with LVM and LVH in men, but not in women. These findings are in line with previously reported sex-specific patterns of cardiac remodeling [101132]. In a previous cross-sectional study among 2,531 men with sexual dysfunction, low serum prolactin concentrations were associated with an adverse cardiometabolic profile including higher BMI, unfavorable lipid profile and higher prevalence of T2DM [33]. Additionally, Corona et al. [34] showed inverse associations of prolactin with an unhealthy metabolic phenotype and the metabolic syndrome in middle-aged and elderly men.
There are few potential explanations for the association of low prolactin concentrations with adverse cardiac remodeling in men since epidemiological studies about the cardiometabolic role of prolactin in men are scarce. Karino et al. [35] confirmed that higher total WBC, granulocyte, and neutrophil counts were associated with higher risk of incident coronary heart disease in a population of elderly Japanese-American men; supporting an association between inflammation and cardiovascular disease risk. This finding suggests that the unfavorable cardiometabolic risk profile associated with low prolactin concentrations in men may explain the adverse cardiac remodeling; however, in the present study population, lower serum prolactin was associated with adverse cardiac remodeling independently from other known risk factors.
The association between prolactin and sex hormones may be responsible for the association between prolactin and LV remodeling. The impact of estrogens on prolactin secretion is still not completely clear, partly because of non-physiological experiments and partly because of correlation studies that do not prove a causal role. So, the need for additional studies to explain this association may be warranted.
A potential role for prolactin in cardiac remodeling has been speculated since its 16 kDa N-terminal fragment was identified as a potential co-factor in the pathogenesis of peripartum cardiomyopathy [36], a disease characterized by LV systolic dysfunction and heart failure [37]. The proposed mechanism is unbalanced oxidative stress leading to activation of the protease cathepsin D, which acts to cleave full length 23 kDa prolactin to an angiostatic and proapoptotic 16 kDa form [37].
Prolactin activates the expression of signal transducer and activator of transcription 3 (STAT3) by means of its specific receptors in cardiomyocytes in the heart [36]. STAT3 has several cardioprotective functions in the heart, including protective effects against oxidative stress. Accordingly, the absence of cardioprotective systems like STAT3 could promote the fragmentation of prolactin into its 16 kDa component; thereby, leading to defective cardiac angiogenesis, heart failure, and subsequent mortality [3839]. Halkein et al. [40] explore signaling downstream of prolactin fragment and demonstrate that microRNA-146a is a critical mediator of the antiangiogenic effects in endothelial cells, this study uncovers unexpected exosomal transfer of this microRNA to cardiomyocytes that may affect myocardial metabolism.
However, several limitations of the present investigation merit consideration. Firstly, we did not measure sex hormones or biomarkers of oxidative stress which may have influenced prolactin. Secondly, the generalizability of our results to other ethnicities and age groups is unknown. However, further large prospective studies in multiple ethnic groups are needed to confirm if serum prolactin could be considered a predictor of cardiac morbidity and mortality in patients with prediabetes.
In prediabetes, physiologically low serum prolactin is an independent predictor of increased LVM and LVH in adult men, but not in women. Prolactin may be a potential diagnostic biomarker for cardiac remodeling in adult men with prediabetes.


 XML Download
XML Download