

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Diabetes mellitus is a common metabolic condition resulting in hyperglycemia and hyperglycemia related chronic complications [12]. Due to changes in lifestyle and diet, diabetes has a relatively high prevalence worldwide [3456]. According to the World Health Organization, 170 million people with diabetes lived in 2000, which is estimated to be doubled by 2030 [7]. This disorder results in several acute and chronic micro- and macrovascular complications that decrease the patients' quality of life and increase their morbidity and mortality. These patients consume a large part of healthcare system's budget (i.e., about 14% in the United States [258]. Timely diagnosis and management of diabetes can prevent complications of the disease and improve the patients' quality of life [59].
Despite considerable advances in diagnosis and management of diabetes, there is a large gap between ideal treatment goals and actual outcomes. Lack of up-to-date knowledge, wrong attitudes and malpractice among healthcare workers regarding diabetes control may play an important role in failure to achieve therapeutic goals [10]. In addition, some of the studies showed that patient's knowledge and compliance with treatment regimens are not enough [911]. Studies also showed that the patients' compliance with treatment is not only affected by physicians' behavior, but also by physicians' knowledge and performance in patient education [91112131415].
Due to the crucial roles of physicians in diagnosis, management and education of patients with diabetes [1617], a number of studies investigated the general practitioners and family physicians' knowledge, attitude, and practice (KAP) on diabetes management and reported that physicians have not sufficient knowledge on diabetes care and up-to-date caring guidelines [12171819]. However, studies on internists' KAP on diabetes management are limited [20]. This study aimed to investigate the Iranian internists' KAP on diabetes mellitus and its management.
METHODS
A cross-sectional study was conducted on a random sample of internists who participated in the 26th annual congress of internists in Tehran, Iran on May 2015. The sample size was calculated 93 samples using Stata version 11.0 software (Stata Corp., College Station, TX, USA), based on power of 0.80, α<0.05, effect size=0.1 and an estimation of 60% for the optimum physicians' KAP [12161718]. However, we recruited 100 subjects in the study. Then, using the list of members of Iranian Society of Internists who participated in the congress, a total of 100 internists with inclusion criteria were selected through a simple random sampling method. Internists having at least 2 years of clinical experience as a specialist, and visiting more than 50 patients with diabetes per month were included. Those with a subspecialty degree and those with specialties other than internal medicine were not included in the study.
The study instrument
A two-part researcher made instrument was used. The first part included questions on the subjects' demographics and seven questions on time since graduation in general medicine/specialty, having a stable job in teaching hospitals, participation in continuing medical education (CME) programs related to diabetes during the past year, working at a diabetes clinic, number of patients with diabetes visited in a week, and history of diabetes in a first-degree relative. The second part was designed according to the last American Diabetes Association criteria [5] and is composed of 33 questions on the subjects' knowledge (14 questions), attitude (nine questions), and practice (10 questions). Questions related to knowledge and practice were in multiple choice format with a correct and three wrong choices, and scored as wrong (0) or correct (1). Questions related to attitude were on a five-option Likert scale namely strongly agree, agree, no idea, disagree, and strongly disagree, receiving a score from -2 to 2, respectively. Thus, the minimum and maximum scores were between 0 to 14, 0 to 10, and -18 to 18 for knowledge, practice and attitude parts, respectively. The scores were changed to percentages by dividing the total score of each part to its max score.
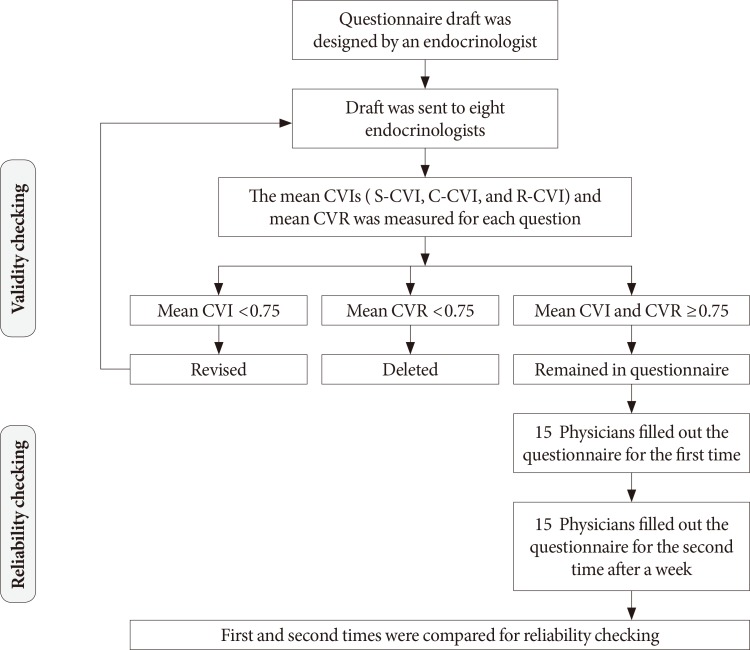
To confirm the content validity of the instrument, eight endocrinologists were asked to rate all questions it terms of necessity, relevance, clarity, and simplicity. Then, content validity index (CVI) and content validity ratio (CVR) of the instrument was calculated. The overall CVI and R-CVI, C-CVI, and S-CVI were 0.888, 0.882, 0.923, and 0.859, respectively. The critical point for the CVR was set as 0.75 according to the Lawshe's table, none of the items had a CVR and less than 0.75 and the CVR of the individual questions ranged between 0.792 and 1. Reliability of the instrument was also assessed through internal consistency method after it was completed by 15 physicians. The Cronbach's alpha was 0.823 for the total instrument and 0.802, 0.791, and 0.845 for the KAP subscales, respectively. The total process of instrument validating is shown in Fig. 1.
All of the participating physicians individually responded the study instrument in a private setting before the congress's formal program is started.
Ethical consideration
This study was approved by the Ethics Committee of Shahid Beheshti University of Medical Sciences (149th session, unique code: IR.SBMU.REC.1392.732). Permissions were sought from the university and authorities of the congress. Enrollment in the study was voluntary, all of the subjects signed an informed consent and assured of anonymity and confidentiality of the data and all the information was kept secure and anonymous.
Statistical analysis
Statistical analysis was performed using SPSS version 21 (IBM Co., Armonk, NY, USA). Descriptive statistics such as percentages, frequencies mean±standard deviation were calculated. The Kolmogorov-Smirnov test was used to examine the normal distribution of quantitative variables. For the quantitative variables that were normally distributed, independent samples t-test was used to compare the mean scores in terms of the subjects' dichotomous personal characteristics. Otherwise, the Mann-Whitney U test was utilized. Chi-square test was also used to compare the nominal or categorical variables. Moreover, the Pearson or Spearman's rank correlation coefficients were calculated to examine the correlation between normally distributed or non-normal variables, respectively. P values less than 0.05 were considered as statistically significant.
RESULTS
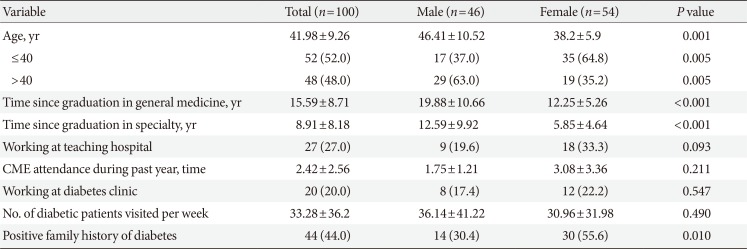
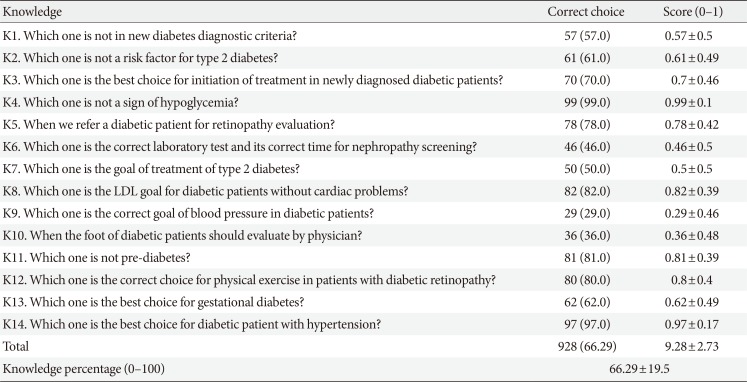
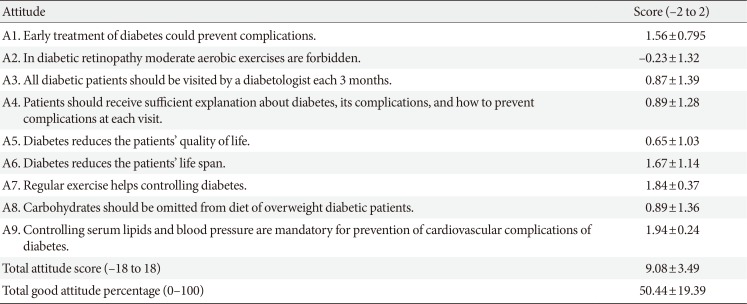
A total 100 internists with the mean age of 41.98±9.26 years were evaluated. Among the subjects, 46% were males. The mean times since graduation in general medicine and specialty were 15.59±8.71 and 8.91±8.18 years, respectively. Mean age, mean time since graduation in general medicine and specialty were significantly more in male physicians than in female ones (P<0.05). Forty-four physicians had a positive family history of diabetes, and female physicians had more family history of diabetes than males (P=0.01). However, no significant differences were found between male and female physicians regarding other personal characteristics (Table 1). Totally, the physicians possessed 66.29%±19.5%, 50.44%±19.39%, and 64.5%±15.3% of the scores in KAP subscales, respectively (Tables 2, 3, 4).
Factors affecting physicians' knowledge, attitude, and practice
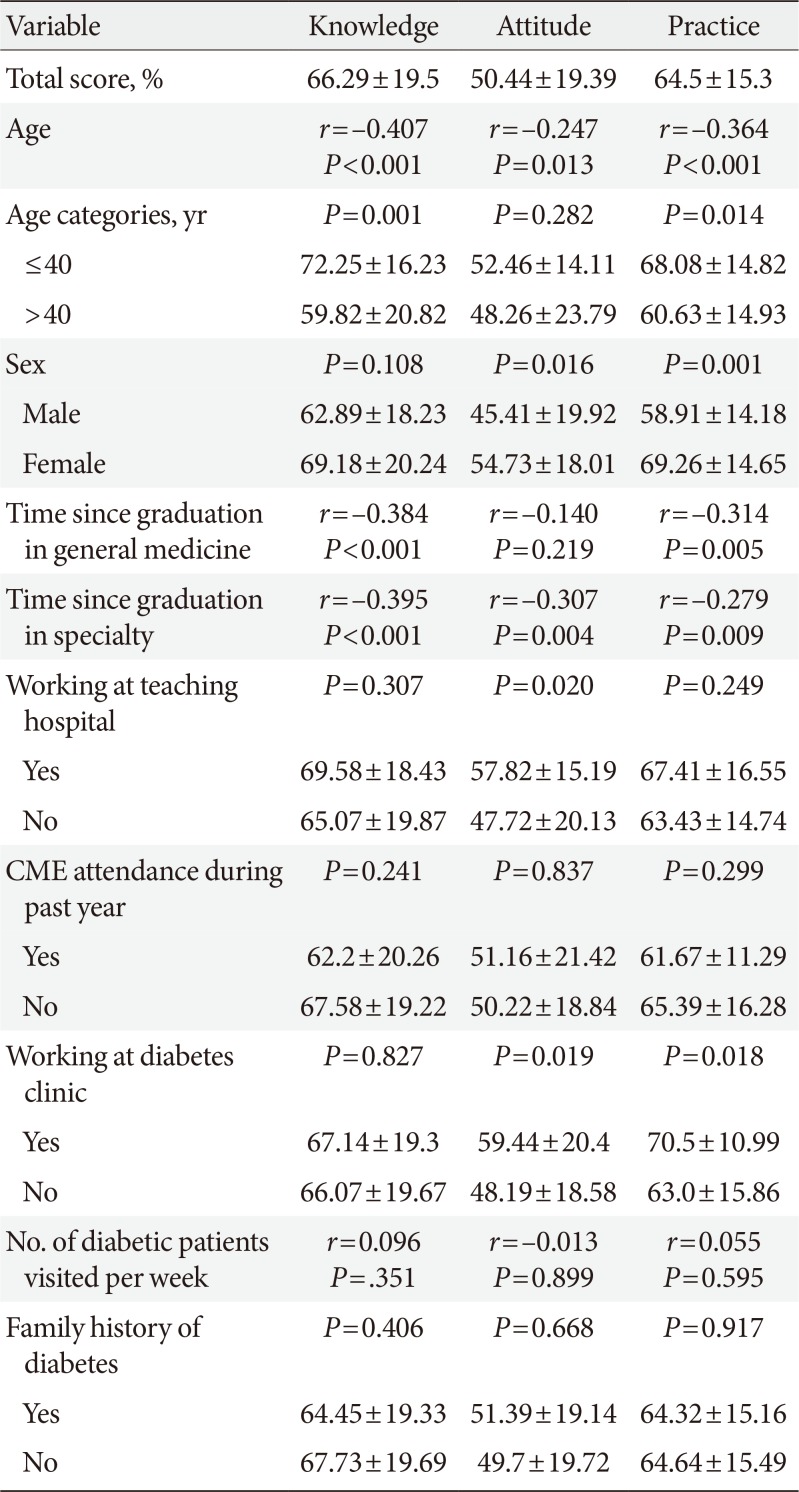
The mean KAP scores were higher in female physicians than males (P<0.05) (Table 5), but age-adjusted analysis showed no significant differences between male and female physicians (P>0.05). The subjects' age showed significant negative correlation with their knowledge (r=-0.407, P<0.001), attitude (r=-0.247, P=0.013), and practice (r=-0.364, P<0.001). The time since graduation in general medicine was inversely correlated with physicians' knowledge (r=-0.384, P<0.001), and practice (r=-0.314, P=0.005) (Table 5). These correlations (between KAP levels and time since graduation in general medicine) were not statistically significant when controlled by the subjects' age (P>0.05). The physicians' KAP were also inversely correlated with time since graduation in specialty (P<0.05) (Table 5). Age-adjusted analyses showed significant correlation only between practice and time since graduation in specialty (r=-0.285, P=0.008).
The level of attitude was significantly higher in physicians working at teaching hospitals in comparison with those who were not working at teaching hospitals (57.82 vs. 47.72, P=0.020). Attitude, and practice scores were significantly higher in physicians who were working at diabetes clinic (P<0.05) (Table 5).
DISCUSSION
In the present study physicians possessed 66.29% of the optimal knowledge level that is expected for an internist to have about diabetes management. They also possessed 50.44% of the optimal attitude and 64.5% of the optimum in the practice subscale. Sex had no significant effect on KAP. The physicians' KAP were inversely correlated with the subjects' age and decreased by increasing in age. Although time since graduation in general medicine and specialty were inversely correlated with subjects' knowledge and practice, but these correlations were along with the subjects' age. Physicians who served in teaching hospitals had a significantly higher attitude than those who did work in such settings. Furthermore, no significant relationship was found between participating in CME programs and the physicians' KAP on diabetes management.
Shera et al. [17] studied diabetes related KAP of family physicians in Pakistan and reported the positive impact of physicians' service years on their knowledge and attitude regarding diabetes management. They also reported that physicians who were working in urban regions had better attitude and practice than those in rural areas [17]. However, in another study, Gosmanova and Gosmanov [20] examined the diabetes-related knowledge of internal medicine residents, and the mean response rate was 87% among their study population, measured by a different instrument. They also compared the level of knowledge among the medical students, and postgraduate students in years 1, 2, 3, and 4. They mentioned a positive trend of knowledge by increasing the year of education, but this trend was not statistically significant [20].
In another study by Mabrouk et al. [18], diabetic neuropathy related KAP was evaluated in 60 family physicians. Nearly half of these family physicians successfully passed the knowledge part, attitude was favorable in 66.7% of physicians, and 43.3% had appropriate practice regarding diabetic neuropathy. In this study, the experience years was correlated with their practice [18].
Peimani et al. [19] also evaluated KAP regarding diabetes in 69 physicians with various specialties. They mentioned a negative linear correlation between KAP score and specialized degree or increased year of practice. The KAP level was not satisfying in their study and they suggested holding CME programs for increasing the KAP regarding diabetes in Iranian physicians [19]. While our study showed no significant differences regarding KAP between subjects participated in a diabetes CME program compared to subjects did not participated in CME programs during the last year. The inconsistencies between studies might be attributed to different factors such as the differences in the study populations, methodologies, and the study instruments. For example the subjects in the Gosmanova and Gosmanov study [20] were internal medicine residents and this group usually much fresh and up-to-date than those who are graduated. However, the subjects in the present study were internists and they are expected to have better KAP on diabetes management. Therefore, our findings signify the need for taking appropriate strategies to improve the internists' KAP on diabetes management.
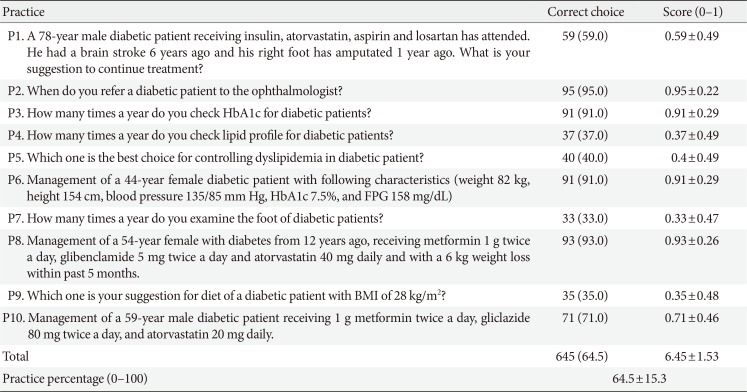
In the present study, the lowest knowledge scores were related to the questions on “optimal blood pressure in patients with diabetes” and “the frequency of diabetic foot examination.” Also the least attitude was about aerobic exercise in patients with diabetic retinopathy and the least practice score was for “the ideal time for diabetic foot examination.” In a previous study in Nigeria, a sample of healthcare workers was evaluated for their knowledge about diabetes and blood pressure. 41.8% of these subjects were physicians, 25.2% were nurses. Of them, 64.1% were aware about the optimum blood sugar in patients with diabetes. Their results showed that physicians who visit more than 50 patients a month or healthcare workers in tertiary level had a higher level of knowledge. However, a majority of the subjects were not aware of the diabetes treatment guidelines [16]. In the present study, we found that physicians with more passed years of graduation have lower knowledge and practice in diabetes management which indicates the necessity of continuous education and evaluation of physicians for diabetes care. An important finding our study was the fact that participation in diabetes education programs did not significantly improve physicians' KAP in diabetes management. This finding signifies that the CME programs are not effective in its current form. Therefore, these programs must be revised in its goals, structure, and contents. Higher attitude and practice of female physicians in the present study is justifiable by higher ages of male physicians.
The present study was the first study which evaluated the KAP of internists who have the main role in diabetes management. Using a valid instrument and also a suitable sample (i.e., those internists with a monthly visit of at least 50 patients with diabetes) was among the strengths of the present study.
The number of members of the Association of Iranian Internists is much higher than our sampling frame, and assessed a sample of the physicians participated in the Annual Congress of Internists. Therefore, selection bias is one of the obvious limitations of this study which may justify the higher level of knowledge of physicians in this study. Another important limitation of the current study is the sample size; therefore, further studies with larger sample sizes are suggested to be conducted. Moreover, this was a cross-sectional study and the causal relationships cannot exactly be examined in this type of studies; therefore, interventional studies and assessing the physicians KAP before and after educational programs are recommended.
According to our results, the KAP level had not significant difference between subjects participated in a CME program compared to subjects did not participated in a CME program during the last year. Hence holding CME programs in current forms seems to be not suitable to increase the KAP regarding diabetes. Subjects' age, time since graduation in general medicine, and specialty were inversely correlated by knowledge and practice. So internists with older age seems to be in priority in these educational programs. Subjects were working in a teaching hospital had better attitude compared to the subjects were not working in these hospitals. Also subjects that were working at a diabetes clinic had better attitude and practice regarding diabetes. Patients with diabetes are advised to be visited by physicians working in the diabetes clinics or teaching hospitals. Approving abovementioned results needs further studies to evaluate the effect of confounders on KAP of physicians more accurately.
 XML Download
XML Download