

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Globally, an estimated 382 million people have diabetes, a number that is expected to rise to 392 million within a generation [1]. In Korea, more than 3 million people have diabetes; the number is increasing rapidly and is expected to reach 6 million by 2050 [2]. Rapid economic development, aging populations, and Westernized lifestyle are factors that contribute to the rise of diabetes in this area [3]. Despite the growing diabetes epidemic, the current treatment of diabetes is not optimal. Only 43.4% of patients with diabetes have been reported to achieve a glycosylated hemoglobin (HbA1c) <7.0% [4], which is similar to data from other Asian countries [5]. In fact, hyperglycemia generally worsens over time primarily due to the progression of β-cell dysfunction [6]. Therefore, treatment strategies are needed to overcome this lack of treatment efficacy.
The current treatment algorithm for type 2 diabetes mellitus (T2DM) recommends initial therapy with lifestyle modifications and metformin administration [78]. The guideline recommends the combination of two or more treatment options if a previous single or combined regimen fails to achieve glycemic goals [78]. Insulin therapy is recommended as the initial treatment if initial HbA1c >9.0% or 10.0% with hyperglycemic symptoms or after metformin failure [9]. However, physicians usually start insulin treatment after two or more oral hypoglycemic agents (OHA) and their combinations have failed [1011]. The main reason for delayed insulin use is that it is an injectable drug that patients often refuse, and it can induce hypoglycemia and weight gain more than other OHAs [12]. However, early insulin therapy could be beneficial in considering the prevention of β-cell dysfunction [13].
The early initiation of insulin therapy has been suggested specifically in patients who were not achieving the glycemic target using combined OHA because OHA showed repeat failure and weak evidence in treatment durability [141516]. The important treatment rationale is that insulin reduces glucotoxicity and helps preserve pancreatic β-cell function for a longer time period than OHA, either alone or in combination [13]. A large meta-analysis of randomized controlled trials in patients with T2DM has shown that ≥50% of patients who had previously uncontrolled disease on zero, one, or two OHAs (baseline HbA1c, 8.7% to 9.1%), achieved HbA1c ≤7.0% after 24 weeks of treatment following the addition of basal insulin [17].
According to the data from clinical trials, individual treatment options, such as maximizing OHAs, adding basal insulin, or initiation of an intensified insulin regimen showed an advantage by lowering glucose; however, real-world data are scarce in patients treated with combination OHAs such as sulfonylurea plus metformin. Hence, this observational study was conducted to evaluate the efficacy of prescribed therapeutic options in patients with T2DM uncontrolled by sulfonylurea plus metformin in actual clinical practice.
METHODS
This open-label, multicenter, non-interventional, prospective, observational disease registry was conducted in 144 non-tertiary hospitals in various districts in Korea from June 2008 to July 2010. This study was conducted in accordance with the ethical principles stated in the Declaration of Helsinki and in compliance with the International Conference on Harmonization-Good Clinical Practice guidelines. Before the start of the study, written informed consent was obtained by the investigators from each patient. The study protocol was approved by the Institutional Review Board of each site (IRB No. B-0808-060-002).
This study included patients with uncontrolled T2DM who had been prescribed sulfonylurea and metformin for at least 3 months and who had HbA1c >7.0% in the last month. Patients currently involved in another trial were excluded from the study. The antidiabetic medication was decided according to the physician's discretion. In the final analysis, subjects were classified into the following three groups according to treatment regimen: intensifying OHAs (group A), adding basal insulin (group B), or starting intensified insulin therapy (group C). The intensified insulin therapy included basal bolus, pre-mixed insulin, and continuous subcutaneous insulin infusion.
This study was scheduled for a period of 6 months after a change in the patients' treatment regimen. The follow-up period was 6±1 months for each patient. The following three prospective visits were planned: visit 1 (recruitment date), visit 2 (3±1 months), and visit 3 (6±1 months). Any additional visits during the 6-month period were adjusted to the closest visit in the three-visit schedule. For patients who did not attend visit 3, visit 2 was recorded as the last visit.
Data were recorded by investigators for variables including patient baseline demographics, HbA1c, body weight, and fasting plasma glucose (FPG) levels at all visits. The number of patients by type of prescription was also recorded at all visits. Because this study was a non-interventional, observational registry, safety data were spontaneously and voluntarily collected based on investigator judgment. For analysis of safety data, we reviewed medical chart notes.
Statistical analysis
Descriptive statistics were provided for all collected variables. Categorical data were summarized as frequency and percentage, and quantitative data were summarized as mean±standard deviation. Baseline characteristics were analyzed with analysis of variance and post hoc analysis was performed using Scheffe's test. The change in the HbA1c, FPG, and body weight from baseline to the end of the study according to group was analyzed by analysis of covariance with adjusted baseline values. The glycemic control rate was defined as the proportion of patients who achieved target HbA1c <7.0% or <6.5% and was calculated using chi-square test. The target FPG was <130 mg/dL according to the treatment guideline of the Korean Diabetes Association [8]. All statistical analyses were performed with SAS software version 9.2 (SAS Institute Inc., Cary, NC, USA). For patients whose data at 6 months post-baseline were not collected, visit 2 was used as the last visit.
RESULTS
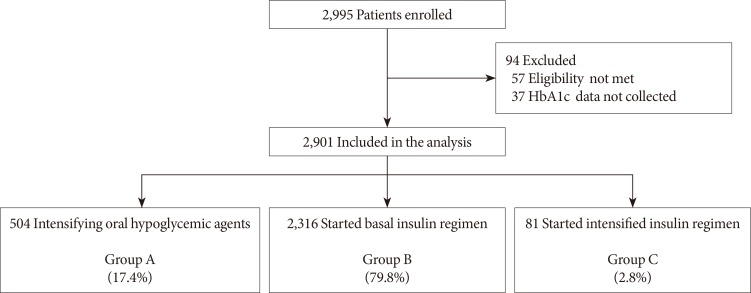
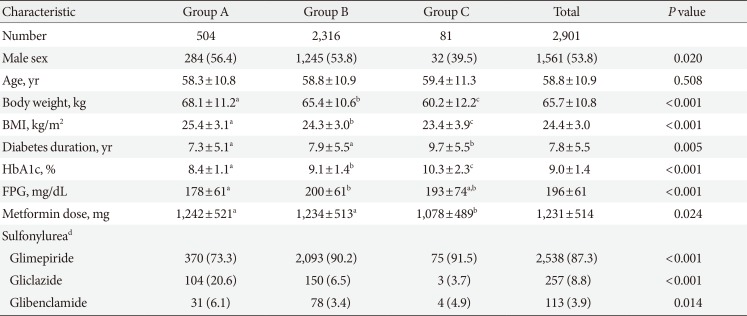
Of the total 2,995 patients enrolled, 94 patients were excluded from the analysis due to a violation of inclusion criteria (57 patients) and HbA1c data not being collected (37 patients). Finally, data from 2,901 patients were analyzed (Fig. 1). There were 504 (17.4%), 2,316 (79.8%), and 81 patients (2.8%) in groups A, B, and C, respectively. The mean age of the study population was 58.8±10.9 years, and the mean duration of diabetes was 7.8±5.5 years (Table 1). Patients in group C showed higher levels of HbA1c, lower body mass index (BMI), and longer duration of diabetes at baseline. The mean dose of metformin was approximately 1,200 mg per day, but the dose prescribed to group C was relatively lower than other groups. Glimepiride was the most commonly prescribed sulfonylurea followed by gliclazide and glibenclamide. The starting daily insulin doses were 15.4±6.7 IU in group B and 37.6±11.4 IU in group C (P<0.001). In group C, pre-mixed insulin, basal plus rapid-acting insulin, and other insulin regimens including continuous insulin treatment or basal bolus insulin were prescribed in 8, 50, and 23 patients, respectively.
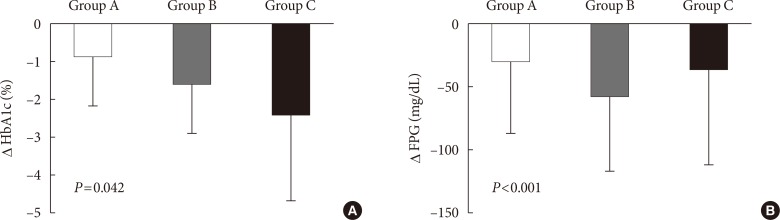
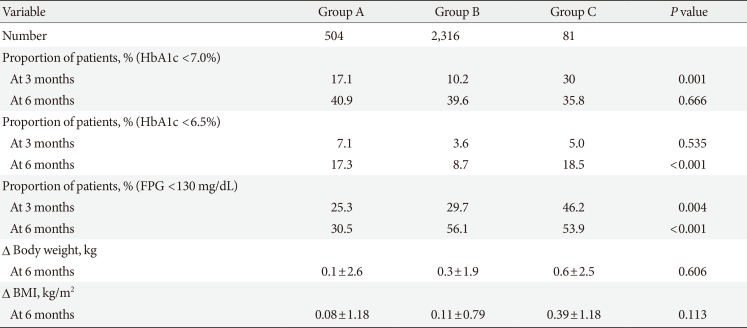
The mean follow-up period from baseline to study end was 6.1±1.0 months. At the second visit (3 months), 2,228 patients were followed, and among them, 24 patients did not attend the 6-month visit. In the final analysis, we used the final data collected at visit 2 in 15 (3.0%), 48 (2.1%), and three subjects (3.7%) in group A, B, and C respectively. Changes in HbA1c during the study period in groups A, B, and C were −0.9%±1.3%, −1.6%±1.3%, and −2.4%±2.3%, respectively (P=0.042) (Fig. 2A). Group C was further divided into three groups of practical relevance: pre-mixed insulin (n=8); basal plus rapidacting insulin (n=50); and other treatments, including continuous insulin treatment and basal bolus injection of rapid-acting insulin (n=23). The changes in HbA1c were −1.5%±1.4%, −2.6%±2.3%, and −2.1%±2.6%, respectively (P<0.001). The changes in FPG were −28.8±57.6, −57.6±59.4, and −36.0±75.6 mg/dL in groups A, B, and C, respectively (P<0.001) (Fig. 2B). Overall, 39.7% of patients reached the target HbA1c (<7.0%) and 10.4% of patients reached target HbA1c (<6.5%) after 6 months of treatment. After 3 months of treatment, more patients in group C achieved the target HbA1c <7.0% (30% of patients) and FPG <130 mg/dL (18.5% of patients) (Table 2). The percentages of patients attaining HbA1c <7.0% at 6 months were 40.9%, 39.6%, and 35.8% in groups A, B, and C, respectively (P=0.666) (Table 2). Additionally, the percentages of patients with HbA1c <6.5% were 17.3%, 8.7%, and 18.5% in groups A, B, and C, respectively, at 6 months (P<0.001) (Table 2). There was no significant difference in body weight changes between groups (P=0.606) (Table 2). Three episodes of symptomatic hypoglycemia in one patient in group B were reported during the study period.
DISCUSSION
In this observational study, the majority of patients received initiating basal insulin therapy (group B) after treatment failure with sulfonylurea and metformin, followed by intensifying OHAs (group A), and the initiation of intensified insulin regimens (group C). The FPG-lowering efficacy seemed to be superior in group B, but the mean change in HbA1c level was greatest in group C, followed by group B and then group A (Fig. 2). The control rate of HbA1c <7.0% was similar among groups whereas the control rate of HbA1c <6.5% was superior in group C compared to group B (Table 2).
The United Kingdom Prospective Diabetes Study (UKPDS) showed benefits in microvascular and macrovascular complications with strict glycemic control [1819], and the “treat to target” approach has emerged. According to this goal-oriented approach, the importance of early insulin therapy has been adopted in many treatment guidelines for T2DM, and the intensification strategy using combined treatment was recommended as a priority if the first or second drug therapy failed. However, our data indicated that insulin therapy was likely to be started only after the patient's HbA1c level was relatively high enough in an actual clinical practice, because baseline HbA1c levels were higher in groups B and C than group A. Additionally, the duration of diabetes was the longest in group C, and this finding suggested that there is a clinical inertia in initiating insulin therapy. According to studies of other ethnic groups, there was also a barrier in starting insulin therapy [2021]. Continuous efforts are needed to educate patients and physicians to overcome this gap between guidelines and actual clinical practice. In this context, the results from this study will give us a good evidence for the importance of initiating insulin therapy.
In the current study, the achievement rates of HbA1c target <7.0% were similar among the groups, whereas the percentage of patients in group C achieving a HbA1c target <6.5% was higher compared to that of the other groups (Table 2). We inferred that a significantly higher starting dose of insulin in group C compared to group B might have influenced this difference. Although data are lacking about the types and dosages of insulin, patients in group C might have received a sufficient dose of prandial insulin to control postprandial hyperglycemia. However, because the nature of this study design was that of an observational study, there were significant differences in baseline glucose levels and key clinical parameters among groups. To overcome this limitation, we investigated the difference in glucose-lowering efficacy after adjusting baseline HbA1c and clinical parameters such as gender, body weight (or BMI), and diabetes duration. In this analysis, the significant difference of glucose-lowering efficacy remained. This result may suggest that intensified insulin treatment could be useful for individuals whose HbA1c target is low, such as younger age patients without prior history of cardiovascular disease.
This research was not a randomized clinical trial but an observational study; therefore, a treat-to-target algorithm was not used. Previous studies have explained that the fear of hypoglycemia by both physicians and patients is the main reason for under-titration [2223]. Physicians or patients might not increase the dose of insulin optimally, and this factor could result in low target achievement rates together with few reports of hypoglycemia in our study. However, the glucose-lowering effect was not likely to be inferior compared to the effect in a recently published study that compared treatment with pre-mixed insulin and basal bolus insulin in an Asian population [24]. Although the clinical trial followed study-specific titration algorithms and our study did not, our study showed numerically better glycemic control rates than the above-mentioned study [24]. Therefore, even if insulin treatment was not intensified according to treat-to-target algorithm, initiating insulin treatment might be beneficial in terms of reducing hyperglycemia in actual clinical practice.
Other important points regarding the efficacy of insulin therapy are patient-related factors. Previous observation studies conducted in Korea showed that the greatest glucose-lowering effect was observed using the basal bolus regimen [2526] especially in patients with a high baseline HbA1c (≥9.0%) [25]. In our study, we also observed the greatest glucose-lowering efficacy using intensified insulin regimens (group C), and the patients in group C showed relatively higher baseline HbA1c levels as well as longer duration of diabetes. Even though this study did not compare the efficacy of insulin therapy according to a patient's clinical characteristics, we could speculate that patients with long-lasting diabetes having high HbA1c would be a good candidate for intensified insulin therapy. However, in addition to a greater reduction of hyperglycemia, which was usually followed by reduction of glycosuria [27], there was a trend towards increasing BMI in group C.
In this study, we restricted participants to those receiving metformin and sulfonylurea; whereas other actual clinical studies included patients receiving diverse OHAs [2526]. Therefore, we could minimize the bias driven by variety in OHAs. In addition, the high follow-up rate (97.7%) is another important strength of this study.
The data from the current study should be understood based on a few limitations. First, this study was an observational study. Therefore, the effectiveness between treatment regimens cannot be compared. Instead, this study described the real clinical situation of delayed intensification of antidiabetic treatment and the gap between routine clinical practice and treatment guidelines. Second, there were few adverse events reported, probably due to under-reporting from patients or incomplete medical records. A modest adjustment of insulin dose in actual practice to avoid hypoglycemia might be another reason. Third, we did not collect the data about the final dosage of insulin in detail. Fourth, as various emerging treatments for T2DM have been introduced, other combination treatments with OHAs such as metformin plus a dipeptidyl peptidase-4 inhibitor are widely used. Therefore, further study is needed to evaluate the efficacy and safety of insulin treatment strategies in addition to various combinations of OHAs and intensifying OHAs.
In summary, this study revealed actual clinical practice in which physicians initiated insulin therapy if patients' hyperglycemia reached a relatively high level and the duration of diabetes was relatively long. Finally, intensified insulin therapy might be the most effective treatment for T2DM that does not cause a significant increase in body weight and hypoglycemia compared to combination treatments of OHAs or basal insulin therapy.
 XML Download
XML Download