

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Gastrointestinal (GI) symptoms are common in patients with type 2 diabetes mellitus (T2DM) [1]. These symptoms can influence the patient's health-related quality of life and affect dietary habits, productivity, and employment status [23]. The prevalence of gastroesophageal reflux disease (GERD) is reported as 10% to 20% in Western countries [45], whereas Asian countries have a lower prevalence. However, recent studies have shown that the prevalence of GERD is increasing in Asia [46]. A Korean study reported a prevalence of 18% for erosive esophagitis among patients with diabetes mellitus (DM) who underwent esophagogastroduodenoscopy (EGD) due to various GI symptoms [7].
An association is suspected between GI symptoms and DM complications (autonomic neuropathy, peripheral neuropathy, and microvascular complications) and poor glycemic control in patients with DM [8910]. Some studies have shown that T2DM is a risk factor for symptomatic GERD [11], and a higher prevalence (28%) of abnormal GE reflux appeared among asymptomatic diabetic patients than among the general population [12]. However, this relationship is still debated, and the pathogenesis of GERD in T2DM is not yet fully understood.
The aim of this study was to analyze the prevalence and risk factors (including peripheral and cardiovascular autonomic neuropathy) of GERD in Korean patients with T2DM.
METHODS
Study population
This study received the approval of the Clinical Ethics Committee (BSM 2010-03). The research subjects included patients with T2DM and a healthy control group, all over 40 years of age, who received a general checkup (including public corporation checkup) during the period between March 2010 and December 2010 and who provided informed consent for data usage.
Exclusion criteria included stomach or esophagus diseases found by endoscopy during the previous 6 months, current treatment with a gastric acid blocker, cardiovascular diseases or severe heart diseases (hospitalization due to cardiac infarction, stroke, or heart failure during the previous 3 months), renal diseases (creatinine over 2.0 mg/dL), type 1 diabetes, and failure to acquire consent. This study was designed by the division of endocrinology and metabolism at Busan St. Mary's Hospital, and informed consent was received by the Division of Endocrinology and Metabolism and other departments (the Health Examination Center, etc.). Due to a lack of active cooperation with other departments, the number of control group patients who provided informed consent was less than that of patients with T2DM, and this threshold resulted in a discrepancy of age and gender, etc., between T2DM patients and control group patients.
Study protocol
General anthropometry items (height, weight, waist measurement, and blood pressure), smoking and alcohol consumption history, and past and current medical histories were examined for all subjects. The subjects fasted for 8 hours and underwent blood tests in a public corporation checkup (fasting blood glucose, lipid profile, aspartate aminotransferase [AST], alanine aminotransferase [ALT], gamma-glutamyltranspeptidase (γ-GTP), and creatinine) and an upper GI endoscopy. The diabetes patients were also assessed for diabetes duration, glycosylated hemoglobin (HbA1c), complications (autonomic nerve disorder, peripheral nerve disorder, macrovascular complications, peripheral arteriosclerosis, diabetic retinopathy, and diabetic nephropathy), and any current medications.
Diagnosis of gastroesophageal reflux disease
All patients underwent an EGD. All study procedures were performed by five expert endoscopists who had each more than 1,000 endoscopies per year. The experts looked for esophageal mucosal breaks. Reflux esophagitis was graded using the Los Angeles (LA) classification (Supplementary Table 1) [13]. Later, endoscopists were asked to decode the pictures, and the differences are shown in Table 1. In this study, the interobserver reliability of the endoscope result was included in substantial agreement (κ=0.703, P<0.001).
All patients completed a frequency scale for symptoms of GERD (FSSG) questionnaire to assess GERD symptoms. The FSSG consisted of 12 questions, scored to indicate the frequency of symptoms as follows: never, 0; occasionally, 1; sometimes, 2; often, 3; and always, 4. Patients with FSSG scores of more than 8 were considered positive for GERD. When the cut-off score is set at 8 points, this test shows a sensitivity of 62%, a specificity of 59%, and an accuracy of 60% (Supplementary Table 2) [14]. In this study, GERD was diagnosed when a patient had erosive esophagitis or nonerosive esophagitis with an FSSG score ≥8 and minimal change.
Diagnosis of cardiovascular autonomic neuropathy
The cardiovascular autonomic nervous function test was conducted using the DiCAN method (Medicore, Seoul, Korea), which was similar to the method used in our previous research [16]. Measurements included the heart rate change during a Valsalva maneuver, posture change, and repetitive exhalation and inhalation, as well as the blood pressure change during standing and grasping power injection. The scores for these five items were 0 for normal, 0.5 for borderline anomaly, and 1 for anomaly, where a score of 5 was defined as the maximum value. Any case with a total score over 1.5 was defined as having a cardiovascular autonomic nervous disease [16].
Diagnosis of peripheral neuropathy
All neurologic examinations were performed using our previously published algorithms [15]. The total symptom score (TSS) was based on the severity and frequency of pain, burning, paresthesia, and numbness. Symptom scores were summed, and the TSSs ranged from 0 to 14.64 (Supplementary Table 3). A monofilament examination, ankle reflex test, and vibration test were performed to evaluate sensory function.
Patients with a TSS of at least 2 and who showed abnormal sensory function tests were defined as having probable peripheral neuropathy. Patients who had symptoms or abnormal tests were defined as having possible peripheral neuropathy.
Statistical methods
Statistical analyses were performed using SPSS version 14.0 (SPSS Inc., Chicago, IL, USA). Data were expressed as mean±standard error. An independent t-test or chi-square test was used to make comparisons between the groups. Continuous variables were tested with an independent t-test, and discrete variables were tested with a chi-square test. A P value less than 0.05 was considered statistically significant.
RESULTS
Patient characteristics
A total of 442 participants were included in this study. The participants were divided into T2DM patients (n=258) and controls (n=184). The characteristics of each group are summarized in Table 2.
The mean age of patients was higher (57.7±0.6 years vs. 52.7±0.6 years, P<0.001), body mass index (BMI) was higher (25.1±0.2 vs. 23.4±0.2, P<0.001), and cigarette use was more frequent (24% vs. 11%, P=0.008) in the patient group. Systolic blood pressure was also higher (132.2±15.3 mm Hg vs. 124.8±14.1 mm Hg, P<0.001) in the patient group. Diastolic pressure was not significantly different between the two groups (78.4±8.9 mm Hg vs. 76.5±9.8 mm Hg, P=0.101). Laboratory tests showed that total cholesterol (160.1±42.1 vs. 196.5±37.5, P<0.001) and high density lipoprotein cholesterol (46.4±11.4 vs. 53.6±15.2, P<0.001) were lower and triglycerides (135.8±83.9 vs. 129.5±72.1, P<0.001) and fasting plasma glucose (126.9±37.2 vs. 100.9±20.4, P<0.001) were higher in the T2DM patient group. No significant differences were noted in gender, weight, height, alcohol consumption, AST, ALT, or γ-GTP.
GERD and GERD symptoms
The prevalence of GERD showed no difference between the T2DM patient group and the control group (32.6% vs. 35.9%, P=0.266). In endoscopic diagnosis, LA grade A or higher indicated no difference between the two groups either (15.5% vs. 15.7%, P=0.453). Because of the significant differences in age, BMI, and cigarette use between the T2DM patient group and the control group, a Cochran-Mantel-Haenzel test was conducted using an age of 60, BMI of 25, and cigarette use. However, the prevalence of GERD still showed no difference after the revision for risk factors such as age, BMI, and cigarette use, as shown in Table 3.
The prevalence of GERD symptoms also showed no significant difference between the two groups (58.8% vs. 59.2%, P= 0.503) (Table 3).
GERD group and non-GERD group
This study evaluated the differences in clinical characteristics between the GERD group (n=150) and the non-GERD group (n=292) (Table 4). No significant differences were noted between the two groups, which had similar rates of T2DM (56.0% vs. 60.0%, P=0.470), waist measurements (or circumferences; 82.2±8.9 cm vs. 84.1±9.2 cm, P=0.064), BMI (23.9±0.3 vs. 24.8±0.2, P=0.026), rates of cigarette use (16.0% vs. 21.0%, P=0.227), and rates of alcohol consumption (35.0% vs. 38.0%, P=0.566). No differences were detected in blood pressure, fasting glucose levels, or lipid levels.
T2DM patients with GERD and T2DM patients without GERD
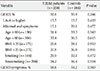
The study also evaluated the differences between T2DM patients with GERD and T2DM patients without GERD (Table 5).
No significant differences were noted in clinical and laboratory characteristics. The mean age (56.8±1.0 years vs. 58.3±0.7 years, P=0.234), BMI (24.5±0.5 vs. 25.4±0.3, P=0.059), and cigarette use (18% vs. 25%, P=0.185) showed no differences. Systolic blood pressure (132.5±1.7 mm Hg vs. 132.1±1.2 mm Hg, P=0.828) and diastolic pressure (80.0±1.0 mm Hg vs. 77.7±0.7 mm Hg, P=0.053) were similar between the two groups. γ-GTP (38.5±5.6 mm Hg vs. 27.7±1.7 mm Hg, P= 0.021) was higher in the DM with GERD group, but alcohol consumption (38% vs. 38%, P=0.966) showed no difference.
The duration of DM (8.7±0.8 years vs. 8.5±0.5 years, P=0.808), HbA1c levels (7.1%±0.1% vs. 7.6%±0.4%, P=0.358), and fasting C-peptide levels (3.4±1.7 ng/mL vs. 2.8±1.0 ng/mL, P=0.765) showed no differences. Peripheral neuropathy was also not significantly different between the two groups (probable: 4.1% vs. 8.5%, P=0.159; possible: 28.5% vs. 20.8%, P=0.140). No differences were detected in the percentage of individual treatment drugs (insulin, sulfonylurea, metformin, thiazolidinedione, dipeptidyl peptidase-4 inhibitor, angiotensin-converting enzyme inhibitor, angiotensin receptor blocker, calcium channel blocker, β-blocker, statin, aspirin, and cilostazol) between T2DM patients with GERD and T2DM patients without GERD. The percentages of DiCAN scores rated 1.5 or higher, retinopathy, and max-baPWV also did not differ statistically.
DISCUSSION
The characteristic symptoms of heartburn or acid regurgitation are critical in the diagnosis of GERD. However, no specific word exists in the Korean language that can precisely express the characteristic "heartburn," so the descriptions of symptoms by patients are very diverse. This complicates the diagnosis of GERD based only on symptoms. GERD patients in Korea also frequently report accompanying atypical symptoms, such as lung pain, throat irritation, and cough, and these symptoms sometimes manifest only in an atypical manner [17]. Hence, objective diagnosis of GERD is important, and this is accomplished in Korea by endoscopy, 24-hour esophageal pH monitoring, and the Bernstein test. Of these methods, endoscopy has very high specificity, at 96%, despite its low sensitivity of 62% to 68% [18]. Diagnosis can be accurate when erosion is observed, and the reliability of GERD diagnosis can be high when correlated with the accompaniment of symptoms in cases of minimal change. In the present study, GERD was defined as LA grade A (or higher) or a minimal change with GERD symptoms.
T2DM has often been identified as a risk factor for GERD occurrence. A study conducted in the United States reported GERD symptoms in approximately 41% of patients with T2DM [9]. Research using a Korean population as a sample determined that 23.1% of T2DM patients complained of typical GERD symptoms [1920]. In other research, upper GI endoscopy on DM patients who complained of gut symptoms revealed erosive esophagitis in 18% of the DM patients, which was a higher percentage than that seen in persons without DM [7]. A recent meta-analysis also reported a correlation between DM and GERD [21]; however, in the present study, the occurrence rate of GERD of 32.6% in the T2DM group and 35.9% in the control group indicated no significant correlation between the presence of diabetes and GERD. Typical GERD symptoms showed a prevalence of 58.8% in the T2DM group and 59.2% in the control group, again indicating no correlation.
Symptoms of GERD are also known risk factors for metabolic syndrome [22]. In fact, overweight or obesity is more commonly observed among T2DM patients. Some studies have indicated that overweight and obesity are also risk factors for symptoms of GERD [112324]. Waist measurements were compared in the present study, but no difference was observed between the GERD and non-GERD groups. Several studies have reported hypertension, dyslipidemia [22], and poor glycemic control [1] as significant factors for the presence of GERD symptoms among T2DM patients. However, no significant differences were noted in blood pressure, lipid levels, fasting glucose level, and HbA1c between the GERD and non-GERD groups in the present study.
Patients with DM and neuropathy more frequently show GI symptoms when compared with DM patients without neuropathy [11]. Recent research reported a higher prevalence of GERD symptoms among DM patients with neuropathy [9], whereas other research has argued that the existence of neuropathy is irrelevant to the GERD symptoms among DM patients, as the prevalence of GERD showed no significant difference between DM patients with neuropathy and DM patients without neuropathy [25]. The present study confirmed that the presence of cardiovascular autonomic neuropathy and peripheral neuropathy in T2DM patients with GERD and T2DM patients without GERD did not affect the prevalence of GERD, with the results indicating similar percentages of TSS ≥2 and abnormal signs (8.5% vs. 4.1%, P=0.159), TSS ≥2 or abnormal signs (28.5% vs. 20.8%, P=0.140), and DiCAN scores of 1.5 or higher (56.0% vs. 55.0%, P=0.894).
The relaxation of the lower esophageal sphincter is held as one reason for GERD, and a variety of medicines are reported to influence this [26]. These medicines include beta-agonists, alpha-adrenergic antagonists, nitrates, calcium channel blockers, anticholinergics, theophylline, morphine, meperidine, diazepam, and barbiturates [26]. Many diabetes patients use calcium channel blockers as hypertension medicines. In this study, however, T2DM patients with GERD showed 25% and those without GERD showed 31% (P=0.380) using calcium channel blockers, indicating no significant difference.
This study was performed on patients who visited Busan St. Mary's Hospital for general checkups (including public corporation checkups). In Korea, the National Health Insurance Service mandates that everyone over age 40 undergo upper gastrointestinography or EGD for the purpose of early diagnosis of stomach cancer, regardless of the presence or absence of symptoms. However, the actual inspection rate for the early diagnosis of stomach cancer in 2009 was 41.3% [27], and 46.9% of the patients who received an early diagnosis of stomach cancer in 2005 visited the hospital for checkups because of the presence of physical symptoms [28], implying the possibility that the test was performed on subjects that showed symptoms. That is, the possibility of overestimation of the prevalence and symptoms of GERD cannot be ruled out in the present study. The present study also has a limitation in that it could not check the factors that influence GERD occurrence, including drugs that affect gastric acid secretion (especially nonsteroidal anti-inflammatory drugs), life habits, and Helicobacter pylori infection. However, the present study has the advantage that every patient underwent EGD and the existence of neuropathy was confirmed through objective testing.
On balance, DM is an unlikely risk factor for GERD symptoms and GERD occurrence. No significant correlation was observed between autonomic or peripheral neuropathy and GERD symptoms and occurrence. Further studies that control for the major factors of GERD occurrence, such as diet and lifestyle, as well as H. pylori infection, will be necessary in the future.




 XML Download
XML Download