

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Age-related macular degeneration (AMD) with subfoveal choroidal neovascularization (CNV) represents one of most common causes of vision loss in elderly populations [1,2,3,4]. Vascular endothelial growth factors (VEGFs) have been implicated as one of the most important factors in the pathogenesis of CNV [4,5,6]. Based on numerous clinical trials, intravitreal ranibizumab injection is considered as a standard treatment for CNV in AMD [5,6,7,8,9]. Unfortunately, information is limited regarding treatment results for CNV and concurrent VEGF-mediated pathologies such as diabetic retinopathy (DR). Due to underlying changes in choriocapillaries and high VEGF concentrations in DR, there might be a different disease course and treatment response for CNV in such cases [9,10,11,12,13,14,15]. However, to the best of our knowledge, there are no reports regarding this treatment in patients who concurrently have the advanced form of these two diseases. In this report, we describe the changes in visual acuity and central subfield thickness (CST) on OCT after the intravitreal administration of ranibizumab for patients with neovascular AMD and severe DR.
METHODS
We retrospectively reviewed 11 diabetic Korean patients with subfoveal CNV from four centers. The patients were diagnosed with severe non-proliferative diabetic retinopathy (NPDR) or proliferative diabetic retinopathy (PDR). The patients underwent initial intravitreal ranibizumab injections between September 2009 and November 2010 and had a follow-up period of at least 6 months. The inclusion criteria were eyes with at least severe NPDR or PDR (regressed PDR and early PDR) with actively leaking subfoveal CNV. DR was graded according to the Early Treatment Diabetic Retinopathy Study severity scale. [16] The exclusion criteria were as follows: (1) neovascular maculopathy associated with angioid streaks or pathological myopia; (2) diabetic patients without apparent DR, mild or moderate NPDR, or other retinal vasculopathy-like retinal vein occlusion; (3) a history of intraocular surgery within 6 months prior to treatment (including cataract surgery); or (4) presence of glaucoma. All patients provided written informed consent. This study adhered to the tenets of the Declaration of Helsinki and was approved by the Institutional Review Board of Kangbuk Samsung Hospital in Seoul, Korea.
CNV was defined according to the Treatment of Age-Related Macular Degeneration with Photodynamic Therapy (TAP) and Verteporfin therapy of subfoveal choroidal neovascularization in pathologic myopia (VIP) trials [17]. Classical CNV and occult CNV with fibrovascular pigment epithelial detachment and late leakage of undetermined origin were included. Each patient underwent an ophthalmic examination including slit-lamp biomicroscopy, indirect ophthalmoscopy, fundus color photography, fluorescein angiography (FA; TRC-NW200; Topcon, Tokyo, Japan), and optical coherence tomography (OCT) software version 4.0.1 (Carl Zeiss Meditec, Dublin, CA, USA; 3D OCT-2000 Spectral Domain OCT, Topcon, CA, USA; and Cirrus HD-OCT, Carl Zeiss Meditec). The patients received three loading doses of ranibizumab (0.5 mg) injection at 1-month intervals. Aseptic technique was used in drug preparation and administration. After the loading period, patients were instructed to return to the clinic in 4 to 6 weeks. If a patient presented with signs of CNV activity, such as a new hemorrhage, edema, or subretinal fluid, an additional injection was performed. Patients without signs of CNV activity on examination were followed at an average interval of 3 months. Clinical characteristics including age, gender distribution, stage of DR, and CNV type were evaluated. Best-corrected visual acuity (BCVA) and CST were measured at every visit, and changes in BCVA and CST from baseline were evaluated at 1, 3, 6, and 12 months after treatment.
Re-evaluation of the patients included BCVA, slit-lamp examination, fundus examination, OCT, and/or FA.
Statistical analyses were performed using IBM SPSS Statistics 19.0 (IBM Co., Armonk, NY, USA). The data are presented as mean±standard deviation. For statistical analysis, BCVA values were converted to logarithm of the minimum angle of resolution (logMAR) scale. Wilcoxon's signed ranks test was performed to examine changed in BCVA or CST from baseline. P values <0.05 were considered as statistically significant.
RESULTS
Eleven eyes from 11 patients were evaluated in this study. There were nine men (81.8%) and two women (18.2%). The mean age of the patients was 70.1±7.3 years with a range of 54 to 83 years (Table 1). Of the 11 eyes, four eyes (36.4%) exhibited severe NPDR, and seven eyes (63.6%) exhibited PDR (Table 1). Eight eyes (72.7%) were treated with pan-retinal photocoagulation prior to the intravitreal ranibizumab injection. Among the seven PDR eyes, three eyes exhibited regressed PDR. Only one eye underwent focal or grid laser photocoagulation prior to the ranibizumab injection. The most common type of CNV was predominantly classical CNV (five eyes, 45.5%), followed by occult CNV (four eyes, 36.4%), then minimally classical CNV (one eye, 9.1%) and PCV (one eye, 9.1%) (Table 1). The mean follow-up period was 16.73±8.89 months, and the mean number of ranibizumab injections was 3.82±0.87 (Table 1).
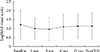
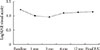
The change of mean BCVA during the follow-up period is shown at Fig. 1. The mean BCVA at baseline was 1.21±0.80 logMAR and improved at 3 months to 1.00±0.59 logMAR (P=0.044). At 6 and 12 months, the mean BCVA improved to 1.10±0.68 logMAR (P=0.0.296) at 6 months, and 1.13±0.66 logMAR (P=0.838) at 12 months; this change was not statistically significant. Although not statistically significant, the mean CST was 343.9±134.6 µm at baseline and changed to 367.8±172.1, 346.2±246.2, 342±194.1, and 294.2±108.3 µm at 1, 3, 6, and 12 months after injection, respectively (Fig. 2). No local or systemic complications were noted in any of the study patients at any time during the follow-up period.
Seven eyes (63.6%), of which, five were from men (71.4%) and two were from women (28.6%), had an improvement in BCVA at 3 months after ranibizumab injection. The mean age was 70.14±4.06 years with a range of 65 to 76 years. Three eyes (42.9%) exhibited severe NPDR, and four (57.1%) exhibited PDR. There were three eyes with predominantly classical CNV, one eye with minimally classical CNV, two eyes with occult with no classical CNV, and only one eye was PCV type. The mean baseline BCVA of the seven eyes, which exhibited visual improvement at 3 months, continued to improve up to 12 months after the injections. The CST in this subgroup increased to 439 µm from baseline (266 µm) after 1 month and decreased to 278, 285, and 234 µm at 3, 6, and 12 months, respectively. However, such changes in CST were not statistically significant.
DISCUSSION
Ranibizumab (Lucentis; Genentech Inc., San Francisco, CA, USA) is a humanized, recombinant antibody fragment that binds to all isoforms of VEGF and is currently approved by the Food and Drug Administration for neovascular AMD. In the Minimally Classic/Occult Trial of the Anti-VEGF Antibody Ranibizumab in the Treatment of Neo-vascular AMD (MARINA) study, the mean increase in visual acuity in the 0.5 mg ranibizumab injection group was 7.2 letters-an improvement that was maintained for 24 months [13]. In the Anti-VEGF Antibody for the Treatment of Predominantly Classic Choroidal Neovascularization in Age-Related Macular Degeneration (ANCHOR) study, visual acuity increased by 5.9 letters in the 0.5 mg group at 1 month and by 8.5 letters at 12 months [14]. At 12 months, visual acuity improved by 15 letters or more in 33.8% of patients in the MARINA study [13] and 40.3% of patients in the ANCHOR study [14]. In our study, eight of the 11 patients (72.7%) gained or had stable vision (mean 0.32 logMAR), and three patients (27.3%) lost one or more lines of vision (mean 0.51 logMAR). However, after 3 months, the improvement in visual acuity did not reach statistical significance. Failure to maintain the improvement of visual acuity after 3 months in some patients can be partially attributed to poor baseline visual acuity and the possibility of underlying microvascular damage from pre-existing DR. Thus, in these patients, monthly ranibizumab injection rather than pro re nata injections might be considered.
The effects of chronic hyperglycemia on the treatment response of subfoveal CNV from AMD combined with severe DR remain unclear. Hyperglycemia might affect pathological changes such as thickening of Bruch's membrane or luminal narrowing and dropout of choriocapillaries that can result in leakage [9]. Ladd et al. [18] reported the effect of photodynamic therapy (PDT) with verteporin in CNV with underlying DR. Four eyes from three patients received PDT, and there was no damage to retinal vessels or progression of DR [18]. In most cases, subretinal fluid or hemorrhage decreased, but fluorescein leakage persisted. After 3 months, visual acuity was stable in two eyes, improved in one eye, and decreased in one eye. In our study, seven of 11 eyes exhibited improved visual acuity at 1 and 3 months after ranivizumab injection. Although it is difficult to directly compare these results, anti-VEGF therapy might be more effective than PDT in patients with DR and AMD. Anti-VEGF therapy might reduce macular edema and the overall severity of retinopathy, restoring the blood-retina barrier by removing angiogenic mediators as previously reported [19].
Classical CNV was the most common form (45.5%) of CNV among AMD patients who also exhibited concurrent severe DR in this study, which was consistent with a previous finding of 42.9% [20]. The incidence of classical CNV was twice as high when compared to other studies of AMD patients, which reported proportions of 20% to 23%. Further investigation is required to determine whether the classical form of CNV is more common in diabetic eyes than in nondiabetic eyes.
A limitation of this study was the small number of patients and the retrospective design. Longitudinal studies with a larger patient cohort must be considered. Further studies measuring local VEGF concentration and dose alteration in these patients might be needed.
In conclusion, there was significant BCVA improvement at 3 months in subfoveal CNV patients with severe DR who were treated with ranibizumab. However, the improvement of visual acuity was not maintained after 3 months. There was a predominance of men and the classical form of CNV. We could not exclude the possibility of the effect of smoking on the male predominance in this study, as we did not collect data regarding smoking status. The improvement in visual acuity and decrease of CST might be limited for eyes with CNV in severe DR. A new strategy for treating neovascular AMD with combined severe DR, such as increasing the concentration of ranibizumab or extending the treatment period, should be considered.

 XML Download
XML Download