

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Obesity is an increasing public health problem that is associated with cardiovascular death [12]. The metabolically deleterious form of obesity is associated with ectopic lipid deposition in multiple tissues, including the heart [345]. Epicardial adipose tissue (EAT) is defined as the adipose tissue between the myocardium and the visceral layer of the pericardium [67]. Epicardial fat covers 80% of the heart's surface and constitutes 20% of the total heart weight. EAT is present along the coronary arteries and over the right ventricle, especially along the acute margin and atrioventricular and interventricular grooves (IVGs) [38]. Because of its anatomical contiguity to the heart, epicardial fat can locally modulate the myocardium and coronary arteries [91011].
Epicardial fat is involved in lipid and energy homeostasis with a substantial capacity for free fatty acid release and uptake and a low rate of glucose utilization [11]. Central obesity and insulin resistance are the key components of metabolic syndrome (MS) [121314]. EAT is a type of visceral adipose tissue that plays an important role in the progression of MS [1516]. The amount of EAT within an individual has been correlated with MS components [71718].
Epicardial fat can be measured with imaging techniques such as echocardiography, cardiac magnetic resonance imaging (MRI), or multidetector computed tomography (MDCT) [11]. MDCT can provide a more accurate measurement of fat around the heart than can other techniques because of its high temporal resolution [19]. Because epicardial fat volume (EFV) measurements require short-axis reformatting and manual tracing of the pericardium, which is time-consuming [5], the epicardial fat area (EFA) was suggested as a simple and quick method for representing EFV [19]. Additionally, measuring the EAT thickness is more convenient and easier than measuring the amount of EAT.
Previous studies have examined the relationship between EAT thickness measured by MDCT and MS [717]. However, no study has investigated the relationship between region-specific EAT thickness measured by MDCT and MS in Korean adults. We aimed to devise a simple method for representing EAT and to examine differences in EAT thickness according to the presence of type 2 diabetes mellitus or obesity in Korean adults.
METHODS
Subjects
We enrolled a total of 94 patients (42.6% with type 2 diabetes mellitus, 53.2% obese, mean age 61±13 years) who were suspected of having coronary artery disease and who underwent MDCT in clinics at Ewha Womans University Mokdong Hospital between March 2012 and June 2013. Subjects were divided into four groups according to presence of type 2 diabetes mellitus or obesity. Diagnoses of type 2 diabetes mellitus were based on American Diabetes Association criteria [20]. Body mass index (BMI) was categorized as <25 and ≥25 kg/m2, which is the cut-off point for obesity in Asian populations [21]. None of our subjects had pericardial effusion. Smoking status was classified as no history of smoking or as a current smoker. Those who had stopped smoking for more than 1 year before the examination were considered to be nonsmokers. The institutional review board of Ewha Womans University Mokdong Hospital approved this study.
Methods
Height and weight were measured for all subjects, and BMI was calculated as weight (kg)/height (m)2. The blood pressure was calculated as the mean of two manual sphygmomanometer readings with the patient in the seated position.
After an overnight fast of at least 8 hours, a venous blood sample was obtained from each subject. The total serum cholesterol, triglycerides, low density lipoprotein cholesterol (LDL-C), and high density lipoprotein cholesterol (HDL-C) levels were measured using an enzymatic assay on an automated analyzer (Hitachi 7150 Automatic Chemistry Analyzer; Hitachi, Tokyo, Japan). The fasting glucose levels were measured via the glucose oxidase method (Beckman Model Glucose Analyzer 2; Beckman Instruments, Fullerton, CA, USA). Glycosylated hemoglobin (HbA1c) was measured using high-performance liquid chromatography assays standardized to Diabetes Control and Complications Trial values (Tosoh Corp., Kyoto, Japan).
All CT images were obtained using a dual-source multidetector row scanner (SOMATOM Definition Flash; Siemens Medical Solutions, Forchheim, Germany). The heart computed tomography (CT) scan was obtained using prospective electrocardiogram gating (step-and-shoot technique). Diastolic images were used for analysis. We analyzed CT images with 0.75-mm thick slices. We were able to clearly identify the pericardium using a dual-source multidetector row scanner. All of the EAT measurements were completed by one radiologist. In a previous study, EFAs at several anatomical landmarks were correlated with the EFV, and the EFA at the left main coronary artery (LMCA) level showed an excellent correlation with EFV [19]. We used the origin of the LMCA as an anatomical landmark to measure EFA (Fig. 1C).
EAT thickness was measured on the parasternal short (Fig. 1A) and horizontal long axis views (Fig. 1B). EAT thickness over the right ventricular (RV) free wall was measured at three equally spaced points along the RV free wall on the basal short-axis plane. The mean of the three measurements was used for analyses. The maximal EAT thickness over the RV free wall was determined from the myocardial surface to the pericardium. The EAT thicknesses over the RV superior wall and left ventricular (LV) lateral wall were measured on the parasternal short axis view. EAT thicknesses in the grooved segments were measured at three sites on the horizontal long-axis plane (right atrioventricular groove [RAVG], left atrioventricular groove [LAVG], and IVG) and at two sites on the basal short-axis plane (superior and inferior IVG). The mean and maximal EAT thicknesses over the RV anterior wall and EAT thicknesses on the RV apex and LV apex were measured on the horizontal long axis view.
Statistical analysis
Statistical analyses were performed using the SPSS version 18.0 (SPSS Inc., Chicago, IL, USA). Data are presented as percentages for categorical variables and as the means±standard deviations for continuous variables. For comparisons of the mean in two groups, we used an unpaired t-test. The chi-square test was used to examine differences among categorical variables. Multigroup comparisons of variables were performed using one-way analysis of variance followed by a Bonferroni correction for post hoc analysis. To adjust the EAT values for BMI between subjects with type 2 diabetes mellitus and subjects without type 2 diabetes mellitus and to adjust the EAT values for type 2 diabetes mellitus status between obese subjects and nonobese subjects, we used analysis of covariance. Correlations between EFA and EAT thickness and between the EAT values and metabolic components were examined by Pearson correlation analysis. To determine the factors associated with EAT thickness in LAVG, a multiple linear regression analysis was performed. Statistical significance was assessed at P<0.05, and then adjusted for multiple comparisons by the Bonferroni method.
RESULTS
The subjects (n=94) had a mean age of 61±13 years. Among them, 42.6% (n=40) had type 2 diabetes mellitus and 53.2% (n=50) were obese. The clinical and biochemical characteristics of the study subjects are shown in Table 1. The mean age; systolic and diastolic blood pressure; total cholesterol, triglycerides, HDL-C, and LDL-C values; presence of plaque or stenosis of coronary arteries by MDCT; and the proportion of current smokers did not differ among the four groups (P>0.05). The proportion of males was highest in the group with type 2 diabetes mellitus and without obesity (75% vs. 33.3%, 38.5%, and 35.7%; P<0.05). The HbA1c values did not significantly differ between the obese subjects and nonobese subjects with type 2 diabetes mellitus (7.3±2.0 vs. 8.4±2.29, P>0.05).
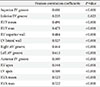
All of the EAT thicknesses were correlated with EFA at the LMCA level (r=0.235 to 0.613, P<0.05), and the EAT thicknesses in the LAVG had the highest correlation coefficient (r=0.613) (Table 2). BMI was positively correlated with EFA at the LMCA level (r=0.411, P<0.001) and the EAT thickness in the LAVG (r=0.450, P<0.001). Systolic and diastolic blood pressure, triglycerides, total cholesterol, LDL-C, gender, and smoking status were not correlated with EFA at the LMCA level or EAT thickness in the LAVG.
The groups with obesity (with or without type 2 diabetes mellitus) had significantly higher EFA values at the level of LMCA than did the group without type 2 diabetes mellitus and obesity (17.0 mm, 13.7 mm vs. 8.4 mm, P<0.05). The group with type 2 diabetes mellitus and obesity had higher EAT thickness values in the RAVG (19.1 mm vs. 16.1 mm) and the LV apex (4.8 mm vs. 3.3 mm) than did the group without type 2 diabetes mellitus and obesity (P<0.05). The group with type 2 diabetes mellitus and obesity had higher EAT thickness values in the LV apex than did the group without type 2 diabetes mellitus and with obesity (4.8 mm vs. 3.5 mm, P<0.05). In addition, the mean EAT thickness in the LAVG was lowest in the group without type 2 diabetes mellitus and obesity (8.8 mm vs. 13.0 mm, 11.8 mm, and 11.8 mm, P<0.05). Except for EAT thicknesses over the RAVG, the LAVG, and the LV apex, the EAT thicknesses did not differ among the four groups (Table 3).
The EAT thicknesses over the LV lateral wall (3.3±1.7 vs. 2.6±1.6), the RAVG (18.0±3.8 vs. 16.2±4.0), and the LAVG (12.0±3.2 vs. 9.9±2.6) in subjects with coronary artery stenosis were greater than in those subjects without coronary artery stenosis by MDCT (P<0.05). Except for the EAT thicknesses over the LV lateral wall, the RAVG, and the LAVG, the EAT thicknesses did not differ between subjects with and without coronary artery stenosis on MDCT. Because our study was a retrospective study, we could not determine the incidence of cardiovascular diseases in our subjects. When we performed the study, 10 subjects (10.6%) were clinically diagnosed with acute coronary syndrome, such as unstable angina, non-ST-elevation myocardial infarction, or ST-elevation myocardial infarction. The EAT thicknesses over the RAVG, the LAVG, and the LV apex in subjects with acute coronary syndrome were greater than in those subjects without acute coronary syndrome (data not shown).
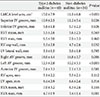
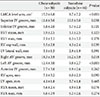
In the group with type 2 diabetes mellitus, there were no correlations between the EAT values and type 2 diabetes mellitus duration or HbA1c levels. When adjusted for BMI, the EFA values at the LMCA level and the EAT thickness in the RAVG and LAVG and the maximal EAT thickness over the RV anterior wall were higher in the group with type 2 diabetes mellitus than in the group without type 2 diabetes mellitus (P<0.05) (Table 4). When adjusted for type 2 diabetes mellitus, the EFA at the LMCA level and the EAT thicknesses in the RV superior wall, RAVG, and LAVG were higher in the obese group than in the nonobese group (P<0.05) (Table 5).
In multiple linear regression analysis, age, type 2 diabetes mellitus, and BMI were significantly associated with the EAT thickness in LAVG when adjusted for gender, smoking status, systolic blood pressure, triglycerides, and plaque or stenosis of coronary arteries by MDCT (P<0.05) (Table 6).
DISCUSSION
We demonstrated that all of the EAT thicknesses were correlated with the EFA at the LMCA level and that the EAT thicknesses in the LAVG had the highest correlation coefficient. The EAT thickness in the LAVG was significantly associated with type 2 diabetes mellitus and obesity independently.
Precise measurement of EAT is a challenge. Standardized measurement of EFV is difficult due to anatomical variations. The echocardiographic epicardial fat measurement is noninvasive and readily available. However, echocardiography cannot provide an adequate window of all cardiac segments and is inadequate, especially in obese patients. Additionally, this method has poor reproducibility [22]. Because volumetric measurements using MDCT and cardiac MRI are accomplished by manually tracing fat in slices and then summing the individual volume measurements, measurement of the EFV in this manner is time-consuming and cumbersome [23]. In a previous study, EFAs at several anatomical landmarks were correlated with the EFV. Among the EFAs, the EFA at the LMCA level showed an excellent correlation with EFV [19]. In our study, all of the EAT thicknesses measured by MDCT were well correlated with the EFA in LMCA. Measuring the EAT thickness would be a convenient and easy method to measure the amount of EAT.
EAT is a metabolically active organ producing bioactive molecules, free fatty acids, and adiponectin. EAT is suggested to play an important role in the progression of MS. EAT thickness was related to the main anthropometric and clinical parameters of MS [71724252627]. The association between EFV and components of MS was evaluated in patients with type 2 diabetes mellitus [18]. Additionally, the echocardiographic EAT thickness was significantly associated with all of the indices of insulin resistance and glucose intolerance measured in obese subjects [28]. In a study with nondiabetic subjects, the EAT thickness was correlated with fasting plasma glucose [29]. Cardiac steatosis measured with the myocardial triglycerides contents was associated with insulin resistance [3031]. Increased EAT thickness, as assessed by MRI, was an independent risk factor for significant coronary artery stenosis in asymptomatic type 2 diabetes mellitus patients [32]. Consistent with previous studies, we demonstrated that the amount of EAT measured by MDCT was associated with the presence of type 2 diabetes mellitus and obesity. It is possible that the EAT thickness varies according to the severity of diabetes mellitus. However, we did not compare the EAT thickness according to glycemic control status. To the best of our knowledge, no study has examined differences in EAT thicknesses according to glycemic control status. Further studies are required to determine differences in EAT thicknesses according to the severity of diabetes mellitus.
Several studies have examined the EAT thickness in subjects with MS. The relationship between region-specific EAT thickness and MS is controversial. The distribution of EAT is primarily concentrated in the grooves [16]. Previous studies demonstrated that the relationship between EAT measured by MDCT and MS were region-specific and mostly correlated at the LAVG level [3334]. In a separate study, the EAT thicknesses in all of the regions evaluated were correlated with MS parameters [17]. The results of our study demonstrated that the EAT thickness, especially in the LAVG, was associated with type 2 diabetes mellitus and obesity. In particular, the EAT thickness in the LAVG was highly correlated with EFA. The relationships between the EAT thickness and type 2 diabetes mellitus as well as obesity can be attributed to the amount of fat accumulated in the LAVG. Because there is a substantial amount of fat around the great cardiac vein traversing the LAVG, the EAT thickness in the LAVG could be associated with type 2 diabetes mellitus as well as obesity. The distribution of EAT is asymmetric, and the importance of the EAT thicknesses may vary according to the regions. Unlike the results of our study, the EAT thickness at the RAVG, as measured by MRI, was a useful marker for differentiating inflammatory status among obese men with MS [35]. However, the method to measure EAT thicknesses and the subjects were different from those in our study.
A previous study investigated the relationship between the region-specific EAT thickness measured by MDCT with MS components in China [34]. This is the first study to evaluate changes in the region-specific EAT thickness measured by MDCT according to the presence of type 2 diabetes mellitus, and obesity in Korean adults.
Adipose tissue macrophages play an important role in the chronic inflammatory state, such as obesity-associated insulin resistance [33]. EAT has been reported to be the source of inflammatory mediators. Infiltration of inflammatory cells, such as macrophages and CD8-positive T cells and expression of adipocytokines in EAT in subjects with coronary artery disease were greater than in subjects without coronary artery disease [3637]. Because of the presence of these inflammatory mediators in EAT, the EAT thickness in the LAVG could be associated with type 2 diabetes mellitus. Additionally, in our study, the EAT thicknesses over the LAVG and RAVG in subjects with coronary artery stenosis were greater than those in subjects without coronary artery stenosis by MDCT. Further studies including markers of inflammation and adipokines are required to determine the pathophysiologic role of EAT.
However, there are some limitations in this study. First, this is a cross-sectional study, and we could therefore only make assumptions about the possible etiological relationships. Second, waist circumference was not measured, and thus, we could not evaluate the relationship between the EAT thickness and abdominal obesity, which is a key component of MS. Third, we did not measure the markers of inflammation and adipokines, which might give important clues about the pathophysiologic role of EAT. Finally, the sample size of our study population was relatively small and the number of normal subjects in the control group was small.
In conclusion, EAT thickness can be easily measured and is suggested to represent EAT. EAT thickness, especially in the LAVG, may be a useful indicator for type 2 diabetes mellitus and obesity. Further larger and longitudinal studies are needed to elucidate the clinical implications relevant to associations between the EAT thickness and MS components.




 XML Download
XML Download