

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The prevalence of type 2 diabetes has tremendously increased worldwide and in Korea [1-3]. Type 2 diabetes was previously defined using fasting plasma glucose (FPG) and 2-hour plasma glucose (PPG) level measured during an oral glucose tolerance test (OGTT). Glycated hemoglobin (HbA1c) has been used as a glycemic marker of diabetes treatment. In June 2009, the International Expert Committee recommended the use of the HbA1c test with a threshold ≥6.5% to diagnose diabetes, which has since been adopted by the American Diabetes Association [4,5]. The Korean Diabetes Association also recommended HbA1c as a diagnostic test [6]. Using HbA1c to diagnose diabetes may identify additional subjects compared to using only fasting glucose level because the measurements of fasting glucose and HbA1c reflect different aspects of glucose metabolism [4,7-9]. After applying this new recommendation, the prevalence of undiagnosed diabetes increased [10].
Although HbA1c may be affected by red cell turnover and renal function rather than glycemia, HbA1c is still a useful diagnostic method of diabetes because of the many advantages such as reduced intraindividual variability, better stability after collection, and no need for fasting compared with measurement of fasting glucose level [4,5]. In comparison, OGTT is a more difficult and time-consuming test to perform than evaluating HbA1c level. If using FPG only for diagnosis of diabetes, individuals with FPG <126 mg/dL and PPG ≥200 mg/dL may be missed because results from FPG and PPG can show a discordance [11-14]. An advantage of using HbA1c level is that it can be determined by both FPG and PPG exposure [7-9]. If using FPG as well as HbA1c in a large-scale screening survey, subjects with FPG <126 mg/dL and PPG ≥200 mg/dL may be diagnosed with diabetes.
We evaluated the prevalence of diabetes according to FPG only and both FPG and HbA1c levels using data from the Korea National Health and Nutrition Examination Survey (KNHANES). In addition, we investigated the trend of the prevalence of diabetes according to sex and age and estimated the population of patients with diabetes or prediabetes.
METHODS
Data source and subjects
This study was based on data from 2011, the second year of the 5th KNHANES V-2 [15]. The KNHANES is a nationally representative, cross-sectional survey designed to estimate the health and nutritional status of the Korean population as determined by the Division of Health and Nutrition Survey under the Korea Centers for Disease Control and Prevention. This survey used a rolling sampling design with stratified multistage cluster probability sampling. The KNHANES consisted of a health interview survey, health examination survey, and nutrition survey. A stratified, multistage probability sampling was used for the selection of 192 primary sampling units (survey districts), and 3,840 households were extracted and surveyed. A total of 10,589 individuals were sampled for the KNHANES V-2, and 8,518 participated in the survey, for a response rate of 80.4%. Of the 8,518 participants in the health survey, we excluded 2,707 subjects aged <30 years, 1,158 subjects with missing glucose or HbA1c, 476 subjects who fasted for less than 8 hours, and 108 subjects who had not been previously diagnosed by a medical doctor or based on current use of antidiabetic medications. The number of excluded subjects among adults aged ≥30 years was 791. These subjects were more likely to be older, male, and have higher FPG than individuals included in the analysis. Therefore, the prevalence of diabetes may be slightly underestimated because excluded subjects might have a higher risk of diabetes. Finally, 5,020 subjects were included in this analysis (Fig. 1). The total number of adults aged ≥30 years in Korea was estimated to be 31,623,912 (15,442,222 men and 16,181,690 women).
Subjects with a previous diagnosis of diabetes made by a physician or those taking insulin or oral hypoglycemic agents were classified as known diabetes. Newly diagnosed diabetes was defined as individuals with FPG ≥126 mg/dL and/or HbA1c ≥6.5% in the absence of known diabetes. Prediabetes was classified as FPG between 100 and 125 mg/dL and/or HbA1c between 5.7% and 6.4% [5].
All individuals in the survey participated voluntarily, and informed consent was obtained from all participants. The survey protocol was approved by the institutional review board of the Korean Centers for Disease Control and Prevention.
Biochemical measurements
Blood was collected from the antecubital vein of each participant after overnight fasting. The samples were properly processed, refrigerated at 2℃ to 8℃, and transported to the Central Testing Institute in Seoul, Korea. Blood samples were analyzed within 24 hours of transportation. Analysis of fasting glucose was performed using a Hitachi Automatic Analyzer 7600 (Hitachi, Tokyo, Japan). HbA1c level was measured with high performance liquid chromatography-723G7 (Tosoh, Tokyo, Japan). Estimated glomerular filtration rates (eGFRs) were calculated with the Cockcroft-Gault formula [16].
Statistical analysis
The data were analyzed with complex-samples analysis procedures in SPSS version 19.0 (IBM Co., Armonk, NY, USA). We used the KNHANES sampling weight variables with stratification and clustering variables to incorporate sample weights and adjust the analysis for the complex sample design of the survey. Nominal variables were presented as the number of cases and percentage and continuous variables as mean±standard error. In order to compare characteristics of four mutually exclusive groups by FPG and HbA1c, general linear regressions were used for continuous variables. A 2-sided P<0.05 was considered to be statistically significant.
RESULTS
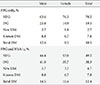
We compared characteristics of the four groups by the presence or absence of FPG ≥126 mg/dL and HbA1c ≥6.5% after excluding cases of known diabetes (Table 1). Most participants were classified into the same group by both FPG and HbA1c; 94.9% of participants were classified as nondiabetic and 1.9% as diabetic. However, discordant classifications occurred for 2.1% of subjects with a HbA1c ≥6.5% and FPG <126 mg/dL and for 1.1% with a HbA1c <6.5% and FPG ≥126 mg/dL. Among the study population, 82.6% of individuals with a HbA1c ≥6.5% and FPG <126 mg/dL had impaired fasting glucose (100 to 125 mg/dL) and 82.9% with a HbA1c <6.5% and FPG ≥126 mg/dL had an HbA1c value between 5.7% to 6.4%. Subjects with HbA1c ≥6.5% and FPG <126 mg/dL were older and had a lower eGFR (P<0.05).
The prevalence of newly diagnosed diabetes was 2.7% using FPG values only (Table 2). If HbA1c was added to the diagnostic measurement, the prevalence of newly diagnosed diabetes increased to 4.7%. The prevalence of diabetes was 10.5% based on FPG only (estimated to be 3.38 million people) and 12.4% based on both FPG and HbA1c (estimated to be 4.01 million people) (Tables 2 and 3). The prevalence of diabetes in male patients increased from 12.6% to 14.5%, and the prevalence of diabetes in female patients increased from 8.5% to 10.4% when including both tests. The percentage of individuals with prediabetes was 19.3% using FPG only (estimated to be 6.1 million people), and that number doubled if HbA1c level was added to FPG value (estimated to be 12.2 million people) (Tables 3 and 4).
The prevalence of diabetes increased with age (Table 3, Fig. 2). Participants aged ≥70 years had diabetes rates of greater than 20%. When HbA1c was used as an additional diagnostic tool of diabetes, the rate of increasing prevalence according to increasing age was high and around by 5% in the group aged ≥70 years. The prevalence of diabetes in males according to age was stable after the age of 50, but the prevalence of diabetes in females was found to continuously increase with age. The prevalence of prediabetes increased even more than the prevalence of diabetes when both FPG and HbA1c tests were used (Table 4, Fig. 3). Prediabetes was largely increased and was found in approximately 50% of subjects aged ≥60 years. HbA1c and FPG levels were highly correlated each other (r=0.820) (Fig. 4).
DISCUSSION
This study showed that an additional 2.1% of participants were diagnosed with diabetes when using HbA1c criteria. This percentage was higher than the 1.2% of participants with HbA1c <6.5% and fasting glucose ≥126 mg/dL among subjects with undiagnosed diabetes. This group may have been living with undiagnosed diabetes for a significant period of time. Therefore, it is thought that chronic hyperglycemia and delays in diagnosis might contribute to reduction of renal function.
As expected, the prevalence of diabetes and prediabetes increased with increasing age. Using HbA1c as a diagnostic tool, elderly patients were more likely to be diagnosed with diabetes and prediabetes. The prevalence of diabetes in elderly patients was higher after including HbA1c level, which partly reflects postprandial hyperglycemia, one of the earliest presentations of diabetes [9,10,17]. Using HbA1c levels ranging from 5.7% to 6.4%, the prevalence of prediabetes was 38.3% of the population, twice as high as the prevalence of prediabetes using FPG criteria alone over all age groups. High levels of HbA1c indicated high risk of subsequent diabetes. It is necessary to determine the optimal cut-off values of HbA1c for prediabetes that may require further intervention and management. This was a tradeoff in that a higher cutoff value would be better for patients at higher risk for the disease but was ultimately not costly. First, the relationship between HbA1c level and increased incidence of diabetes should be clarified with prospective studies in Korea. Next, prediabetic cutoff points of HbA1c must be identified and selected according to capacity for management, budget, and effectiveness of the intervention such as lifestyle modifications [18].
Racial and ethnic differences in HbA1c have been reported [19-22]. In contrast to data of the United States National Health and Nutrition Examination Survey, our data showed that the proportion of participants with HbA1c ≥6.5% and FPG <126 mg/dl was larger than that of participants with HbA1c <6.5% and FPG ≥126 mg/dL among subjects with undiagnosed diabetes [10]. Asians had higher HbA1c levels than whites after adjusting for factors that affected glycemia such as fasting and postload glucose level [19]. Hemoglobin glycation rate, red cell turnover, and other unknown factors may contribute to racial and ethnic differences in HbA1c level [20,23,24]. It is not known, however, if these racial and ethnic differences in HbA1c are related to the risk of microvascular or macrovascular complications. Therefore, an HbA1c threshold of 6.5% should be validated to detect diabetic complications in Korea. For example, the association between hyperglycemia and diabetic retinopathy was the basis for the diagnosis of diabetes [25], and in a cross-sectional cohort study, an HbA1c threshold of 6.5% was appropriate to detect diabetic retinopathy in Korean patients [26]. Further studies are necessary to define the relationship between HbA1c and risk for diabetic complications.
Because of methodological differences among laboratories, the HbA1c assay has been standardized through national programs in the USA, Japan, and Sweden [27-29]. Furthermore, for global standardization of HbA1c measurements, the International Federation of Clinical Chemistry and Laboratory Medicine (IFCC) introduced a new reference method to allow for the conversion of values obtained by previous measurements in different countries [30]. This national and global standardization should be required to adopt HbA1c in the clinical setting and to compare data obtained from many countries. The International HbA1c Consensus Committee recommended that HbA1c results be reported in IFCC units (mmol/mol), derived National Glycohemoglobin Standardization Program units (%), and estimated average glucose level [31].
The strength of our study was that these data were based on a nationwide population that was representative of Korean patients. To our knowledge, this was the first study to investigate the prevalence of diabetes and the characteristics in newly diagnosed diabetes using newly revised recommendation guidelines. This study had some limitations. We raised the issue that prediabetes was largely increased and had a prevalence of almost 40% in the Korean population aged ≥30 years using new diagnostic criteria of diabetes. In a prospective cohort study, the 4-year risk of diabetes in subjects with HbA1c of 5.5% to 6.4% was 2.66 times greater compared to patients with HbA1c level <5.5% [32]. In another prospective, community-based cohort study, an HbA1c cutoff of 5.6% was appropriate for the identification of patients at risk of developing diabetes [33]. Another 4-year longitudinal study showed that an HbA1c cut point of 5.7% was suitable for predicting future cases of diabetes [34]. However, we could not determine an optimal cut point of HbA1c for classifying cases of prediabetes that required further intervention. Finally, OGTTs were not performed in the KNHANES and therefore could be not compared to data collected in this study for the diagnosis of diabetes.
In conclusion, diabetes and prediabetes are largely increased when HbA1c is added as a diagnostic test. Using FPG only can underestimate detection of diabetes and prediabetes. We expect new recommendations to be helpful for detection of subjects with early diabetes at risk for complications. Therefore, we conclude that HbA1c is an appropriate complementary diagnostic diagnostic test for diabetes in Korean patients.







 XML Download
XML Download