

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Nonalcoholic fatty liver disease (NAFLD), characterized by an abnormal accumulation of fat in hepatocytes, is recognized as the most prevalent chronic liver disease in the general population [1], and is increasing rapidly in both Western countries and Asian countries such as Korea [2]. NAFLD is well known to be share the common pathophysiological mechanism of insulin resistance with obesity, metabolic syndrome, and type 2 diabetes [3]. Regarding insulin resistance, the association between NAFLD and visceral fat is well established [4,5]. Koda et al. [6] suggested that visceral fat, not subcutaneous fat, was the most important factor for the development of hepatic steatosis. In addition, many studies have reported that NAFLD could be a risk factor for atherosclerosis and cardiovascular disease [7]. Thus, it is considered to be not only a simple hepatic disease but also a hepatic manifestation of metabolic syndrome [8].
The fatty liver index (FLI) is a simple parameter for the determination of fatty liver, which is easily obtained from body mass index (BMI), waist circumference (WC), triglyceride (TG), and γ-glutamyl transferase (GGT) levels [9]. For high diagnostic accuracy in detecting fatty liver, these parameters were recently validated in large population studies [10,11]. Moreover, higher FLI scores are correlated with an elevated risk for diabetes [12], early carotid atherosclerosis [10], coronary artery disease [13], and all-cause mortality [11].
Skeletal muscle plays an important role in insulin sensitivity as a primary tissue contributing to whole body insulin-mediated glucose uptake [14]. Several findings reported that low skeletal muscle mass is associated with obesity, metabolic syndrome, and dysglycemia [15-17], and the reverse was shown in large populations, with higher muscle mass associated with better insulin resistance and a lower risk of developing diabetes [15]. However, little is known about the relationships between visceral fat and the role of skeletal muscle as a risk factor in NAFLD. The aims of this study are: 1) to determine whether visceral fat is related to FLI; 2) to evaluate the relationship between visceral fat and skeletal muscle mass; and 3) to determine whether skeletal muscle affects the development of NAFLD diagnosed by FLI in Korean subjects.
METHODS
Study population
We reviewed medical records of 11,116 subjects (6,242 males, 4,874 females; mean age, 47.2±10.2 [males] and 46.7±10.9 [females] years) who underwent a health examination at the Yeungnam University Health Promotion Center, Daegu, South Korea between January 2009 and December 2011. We excluded 778 patients who had positive serologic viral hepatitis (hepatitis B surface antigen or anti-hepatitis C virus antibody) and 773 subjects with excessive alcohol consumption (≥20 g/day). After exclusion, there remained 9,565 subjects (5,293 males, 4,272 females). The criteria for the diagnosis of diabetes recommended by the American Diabetes Association [18] were: 1) hemoglobin A1c (HbA1c) ≥6.5%; and 2) fasting plasma glucose (FPG) ≥126 mg/dL (7.0 mmol/L). Adopting International Diabetes Federation (IDF) criteria, metabolic syndrome in South Korean adults was defined by central obesity (waist circumference ≥90 cm for men and ≥85 cm for women) plus two of the following four factors: serum TG ≥150 mg/dL, high density lipoprotein cholesterol (HDL-C) ≤40 mg/dL for men and ≤50 mg/dL for women, systolic blood pressure (SBP) ≥130 mm Hg or diastolic blood pressure (DBP) ≥85 mm Hg, and FPG ≥100 mg/dL [19]. Participants who had antihypertensive medication or were newly diagnosed (SBP ≥140 mm Hg or DBP ≥90 mm Hg) were classified as hypertension group. All patients gave informed consent, and this in turn was approved by the local ethics committee. The study protocol was approved by the Institutional Review Board of Yeungnam University Hospital (YUH-12-0463-O91).
Clinical and laboratory assays
Blood samples were obtained from each individual after a 12-hour overnight fast. Measurement of FPG, bilirubin, aspartate aminotransferase (AST), alanine aminotransferase (ALT), GGT, blood urea nitrogen, and creatinine used the hexokinase method (AU 5400 Autoanalyser; Olympus, Tokyo, Japan). Total cholesterol (TC) was measured using enzyme colorimetry (Kyowa Medex Co., Ltd., Tokyo, Japan), TG was measured using the glycerol elimination method, and HDL-C and low density lipoprotein cholesterol (LDL-C) were measured using direct enzymatic assays (Kyowa Medex Co., Ltd.). HbA1c and microalbuminuria assays were performed using the HLC-723G7 high performance liquid chromatography system (Tosoh, Tokyo, Japan).
Surrogate marker of fatty liver
For determination of nonalcoholic fatty liver, we used a surrogate marker, the FLI [9]. The index uses an algorithm based on BMI, WC, serum TG level, and GGT. It has been validated against hepatic ultrasonography (US) in the general population and has been proven accurate in detecting fatty liver (accuracy, 0.84; 95% confidence interval [CI], 0.81 to 0.87) [9,13]. When FLI is greater than or equal to 60 (FLI ≥60), the probability of having a fatty liver is >78%, and if FLI is <20, the likelihood not to have fatty liver is greater than 91%. A validation of FLI against magnetic resonance spectroscopy demonstrated the presence of hepatic fat (range, 8.6% to 24.0%) in subjects with FLI ≥60 and the absence of hepatic fat in those FLI <20 [13]. Therefore, we categorized our study group into three groups: 1) the low FLI group, FLI <20; 2) the intermediate group, 20≥FLI<60; and 3) the high FLI group, FLI ≥60.
Body composition determined by bioelectric impedance analysis
Waist circumference was measured at the midpoint between the lower border of the rib cage and the iliac crest. We analyzed body composition of all subjects using the Inbody 720 (Biospace, Seoul, Korea), a multifrequency impedance body composition analyzer. The Inbody 720 uses an eight-point tactile electrode method, measuring resistance at five specific frequencies (1, 50, 250, 500 kHz, and 1 MHz) and reactance at three specific frequencies (5, 50, and 250 kHz). We obtained readings for skeletal muscle mass (SMM, kg) and visceral fat area (VFA, cm2). The SMM to VFA ratio (SVR, g/cm2) was calculated as a new index of risk factor for fatty liver by dividing the SMM (g) by VFA (cm2). Skeletal muscle index (SMI) was expressed as percent, dividing the SMM (kg) by total body weight (kg).

Statistical analysis
Quantitative data were expressed as mean±standard deviation, and categorical data were expressed as percentages. The t-tests were used to compare continuous variables, and a χ2 test was used for categorical variables. Analysis of variance (ANOVA) tests were performed to compare continuous variables among FLI groups. Associations between FLI and continuous variables were evaluated by simple and multiple regression analyses. Correlations (Pearson correlation coefficient) and multiple linear regression analyses were also performed. All data analyses were performed using SPSS software for Windows version 14.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
The baseline characteristics of the subjects are shown in Supplementary Table 1. The mean age of males and females were 47.2 and 46.7 years, respectively. Anthropometric values including BMI and WC were significantly higher in males than females. While blood pressure (SBP, DPB), FPG, HbA1c, AST, ALT, GGT, TC, TG, LDL-C, and high sensitivity C-reactive protein (hsCRP) were also higher in the male group, FLI was not significantly different between the male and female groups. The male group showed a higher prevalence of metabolic syndrome, diabetes, and hypertension than the female group. Higher VFA and indexes of skeletal muscle (SMI, SVR, and skeletal muscle-to-total body fat ratio) were identified in the male group, but body fat mass was higher in the female group in bioelectrical impedance analysis (BIA).
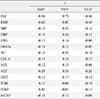
We examined the anthropometric and clinical parameters using the FLI. Table 1 shows that biochemical parameters such as FPG, HbA1c, AST, ALT, TC, LDL-C, and hsCRP increased in the high FLI group compare with other groups, while bilirubin and HDL-C decreased. Compared with the low FLI group (FLI <20) by ANOVA, increased VFA and decreased SMI and SVR were observed in both the high FLI group (FLI ≥60) and the intermediated group (20≤FL<60). There was also an inverse correlation between SMM and VFA in the low FLI group (Fig. 1).
The correlations between several metabolic parameters including FLI and indexes of body composition, such as SMI, SVR, and VFA, are shown in Table 2. Adjusted for age and gender, SMI and SVR correlated negatively with BMI (r=-0.60, r=-0.43, respectively) and FLI (r=-0.56, r=-0.41, respectively), while VFA had a strong positive correlation with FLI (r=0.73).
In simple linear regression analysis (Supplementary Table 2), SVR (males, B=-0.076, β=-0.347; females, B=-0.114, β=-0.569) was shown to significantly affect FLI as a negative factor in both genders. Table 3 shows that in multiple regression analysis, a similar result was obtained, indicating that SVR was an independent factor in FLI and had an inverse correlation (males, B=-0.090, β=-0.408; females, B=-0.085, β=-0.428).
Table 4 displays the odds ratio between NAFLD and SVR. For evaluation of SVR impact on fatty liver, we determined FLD as FLI above 60 and then examined the odds ratio by multiple logistic regression analysis. Among the quartiles, the highest SVR quartile (Q4) had a lower incidence of NAFLD and the odds was 0.038 (95% CI, 0.030 to 0.048) after adjustment for age and gender. In addition, after adjusting for lipid profile, diabetes, hypertension, and hsCRP, we determined that higher quartiles from the lowest quartile group showed a significantly lower odds ratio (Q2, 0.212; Q3, 0.129; Q4, 0.037).
DISCUSSION
In the present study, we found that skeletal muscle and visceral fat contributed to NAFLD. First, the FLI increased in proportion to a rise in VFA and it was consistent with well-established relationships between abdominal obesity and NAFLD. Second, there was an inverse correlation between SMM and VFA. Finally, higher SMM, which is adjusted by visceral fat, was associated with low incidence of NAFLD.
Little is known about how skeletal muscle works on abnormal fat accumulation in internal organs, especially the liver. The role of skeletal muscle has been studied, but is limited to disability and functional activity with aging. However, concerns are growing in the context of insulin resistance. Intuitively, an increase of SMM is expected to give a higher basal metabolic rate and greater energy expenditure, which may in turn lead to reduced weight, including visceral fat and FLD. Recent studies demonstrated that myokines secreted by skeletal muscle prevent systemic inflammation and insulin resistance through antagonizing the proinflammatory and metabolic effect of adipocytes [20]. Even a modest increase in muscle mass was able to prevent not only atherogenesis in prone mice, but also diet-induced obesity and insulin resistance [21]. Large population studies also have been used to characterize metabolic parameters associated with insulin, Srikanthan and Karlamangla [15] showed that higher muscle mass was related with better insulin sensitivity and lower risk of prevalence of transitional/prediabetes or overt diabetes. Physical activity also interrelates with skeletal muscle, even if they are not exactly the same parameters, and higher levels of habitual physical activity are related with a lower intrahepatic fat content [22]. Thus, skeletal muscle has a beneficial effect on the risk of metabolic and cardiovascular disease.
Despite diverse clinical views on the definition of sarcopenia [23], decreased muscle mass is generally accepted as another risk factor of metabolic and cardiovascular disease in the context of insulin resistance. Lu et al. [24] confirmed that sarcopenia as well as obesity affect the development of metabolic syndrome. Kim et al. [16] reported that type 2 diabetes was independently associated with sarcopenia, which was defined using the SMI (%) in Korean patients. Srikanthan et al. [17] reported that sarcopenia might be an early predictor of diabetes susceptibility independent of obesity in the National Health and Nutrition Examination Study III study.
In the present study, the FLI was lower in the group having higher SMM, and simultaneously, the group with NAFLD (FLI ≥60) had lower SMI and higher VFA when compare with the lower FLI group. The lowest SVR quartile group also showed the highest risk of NAFLD. These results are consistent with prior findings and further show that the incidence of NAFLD increases with decreased muscle mass relative to visceral fat (SVR). Thus, skeletal muscle could play a significant role in the development of NAFLD and our results support a favorable role for skeletal muscle in insulin resistance.
We identified an inverse correlation between skeletal muscle and visceral fat. Prior studies showed abdominal obesity negatively affects muscle strength and contributes to the progression of sarcopenia [25], as proinflammatory cytokines and leptin which are secreted by adipocytes stimulate skeletal muscle catabolism and accelerate sarcopenia [26]. Given an increase in fat mass, particularly not subcutaneous but visceral fat, adipocytes overproduce proinflammatory cytokines such as interleukin-6 (IL-6), tumor necrosis factor α, and C-reactive protein [27]. IL-6, a pleiotropic cytokine produced by different tissues and organs, is known to have dual effects on muscle. IL-6 is principally defined as a proinflammatory cytokine, which increases muscle wasting when systemic levels are elevated chronically under persistent inflammatory conditions, cancer, and other chronic disease states. Simultaneously, IL-6 is also one of the few genuine myokines that are produced by and act on skeletal muscle. Muscle induced IL-6 has beneficial effects in muscle growth, regeneration, and regulation of energy metabolism, but its action is transient and short-term [28]. Although the exact mechanisms are not fully understand, we found that skeletal muscle and visceral fat may influence each other in opposition and both strongly contribute to NAFLD. However, we did not directly measure the inflammatory cytokines.
Age-related body composition changes are well documented, and both a progressive increase in fat mass and loss of muscle mass occur even when there are no significant changes in BMI [29]. The change of body composition, especially mass and distribution of fat tissue normally peaks at about age 65 years in men and later in women [30]. We hypothesize that the risk of FLD may increase with aging. However, the result was contrary to what we expected in multiple regression analysis. Even if not significant in women, it is thought to be caused by the relative young age combined with the high BMI of subjects in this study. According to the Korea National Health and Nutrition Examination Survey, the incidence of obesity differed by sex and age in South Korea. The prevalence of obesity (defined by BMI) in men peaks in their 30s (42.3%), next in their 40s (41.2%), and decreases with age. In contrast, the proportion of obese women gradually rises with age (19% in their 30s, 26.7% in their 40s, and highest in their 60s, at 43.3%) [31]. Because participants in this study were in their mid-40s, with above average BMI for the Korean population (defined as overweight by BMI ≥23), obesity may affect their FLI more than age-related changes. Further studies are needed to define the relationship between age and FLD.
Among the methods that assess liver fat accumulation, liver biopsy is the gold standard for evaluating hepatic steatosis and its changes by disease severity. But this procedure is difficult to apply to all patients due to limitations, including its invasiveness, cost, and potential life-threatening complications. Although liver ultrasonography has been used the most widely, low specificity, high cost, and bias of results by the examiner are barriers to use in large populations. Similar shortcomings were observed in other radiologic tests such as computed tomography (CT) and magnetic resonance spectroscopy [32]. Therefore, several methods have been developed for objective assessment of fatty liver, and FLI has been proposed and validated in the general population [10,11]. It can be inferred that factors for calculating the FLI, such as WC, BMI, TG, and GGT, are closely associated with insulin resistance. FLI additionally has advantages in large population studies for providing high accuracy and less error by the examiner. This index showed good predictive value for detection of fatty liver and was validated in studies with the Korean population [33,34]. There are reasons why we used FLI for this study. However, in spite of its many benefits, there are some disadvantages. This surrogate marker does not reflect a histological change of fatty infiltration, and was reported to be a poor predictor of significant steatosis in obese patients (BMI ≥28 kg/m2) [35]. It needs to be validated with various ethnic groups, including Asians, and calibrated for the Asian population because of different definitions of obesity (BMI).
This study has several limitations. First, we did not include the analysis of physical activity. A recent study has shown that exercise reduces the risk of NAFLD and decreases liver enzymes, independent of obesity [36]. Consistent with this study, low physical activity in NAFLD patients was also reported [37]. Because physical activity is closely related to muscle mass, our findings might not be irrelevant, but the cross-sectional design of this study makes it difficult to infer causality between skeletal muscle, visceral fat, and FLD. Second, this study has selection bias because subjects were health check-up participants in a single center. Third, we used the BIA method to measure muscle mass. Though dual energy X-ray absorptiometry or CT were currently gold standard tests for evaluating SMM [38], these methods were limited to epidemiologic studies in terms of cost and time. BIA showed good correlation with the dual energy X-ray absorptiometry method and was also validated in studies of Asians including the Korean population [36,39]. However, overestimation of pathological states such as heart or renal failure may depend on the relationship between body composition and body water content. To minimize overestimation, all participants were required to fast for 8 hours and individuals with renal failure were excluded. Finally, findings from this study can be applied only to Asian populations, but not to other ethnic groups.
In conclusion, VFA is closely correlated with NAFLD diagnosed by FLI. There is an inverse correlation between SMM and VFA. High SMM and low VFA, that is high SVR, is associated with low incidence of NAFLD. These results suggest that body composition, including skeletal muscle, may be more important than simple abdominal obesity in the development of FLD, and concerns about reducing or at least slowing the onset of sarcopenia are needed for prevention.




 XML Download
XML Download