

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The prevalence of obesity in Asia is now an epidemic threat, followed by an exponential increase in the incidence of diabetes [1]. As a result, type 2 diabetes mellitus (T2DM) has become one of the most common metabolic diseases in Korea. Since many epidemiologic, interventional, and laboratory studies have revealed that adequate blood glucose control delays the onset of complications [2-5], there have been continuous efforts toward achieving and maintaining appropriate glucose levels. However, only half of diabetic patients are known to reach glycemic control goals [6]. The highest contributing factor to treatment failure is nonadherence to medications, which is assumed to come from fear of weight gain and hypoglycemia [7-9]. The weight gain and hypoglycemic events are unfortunately common side effects of standard medications.
Exenatide is a recently developed incretin-based medication that is an analog of glucagon-like peptide 1 (GLP-1). GLP-1 is a gut hormone that not only lowers glucose levels by promoting insulin secretion and inhibiting glucagon release, but also controls weight by inducing satiety and slowing gastric emptying time [10,11]. Exenatide achieves better physiological glucose control with low risk of weight gain and hypoglycemia. Therefore, clinicians have turned their attention to exenatide.
Although many exenatide studies have shown good efficacy and safety in diabetic patients, limited information is available from real clinical practice in Korea. Therefore, this retrospective study was designed to analyze the effects of exenatide on blood glucose level and body weight in Korean patients with T2DM.
METHODS
Study subjects
The medical records of the patients who visited Seoul St. Mary's Hospital between June 2009 and October 2011 were screened. The patients were eligible for inclusion in the study if they were Korean, aged 20 to 65 years, and had T2DM for a minimum of 3 months. Subjects were enrolled if their glycated hemoglobin (HbA1c) ≥6.5% and if they did not have any changes in their oral hypoglycemic agents (OHA) for at least 3 months before exenatide was prescribed. Patients were excluded if they had type 1 diabetes with positivity for autoantibodies against glutamic acid decarboxylase, islet cell or insulin, or C-peptide <0.6 ng/mL, gestational diabetes, or diabetes with secondary causes. We also excluded the patients who had significant renal impairment (estimated creatinine clearance <60 mL/min), elevated (more than two-fold the upper limit of normal) alamine aminotransferase or asparatate aminotransferase, or concomitant conditions such as surgery, hospitalization, or cancer, or had used insulin within the previous 3 months. Additional exclusion criteria included switching more than two kinds of OHAs with exenatide treatment, follow-up loss, or discontinuation of exenatide treatment within 6 months.
The patients were subdivided into 4 groups: group 1, an exenatide monotherapy group of treatment-naive patients; group 2, a group of patients who continued their OHA treatments; group 3, a switching group of patients who used exenatide as a substitute for one kind of OHAs; and group 4, a combination group of patients took exenatide along with OHAs.
All patients initially received 5 µg of exenatide twice a day. After 1 month of treatment, the exenatide dosage was increased to 10 µg twice a day. The initial OHAs were maintained for 6 months. Dietitians in the same institute provided individualized medical nutrition therapy and physicians recommended at least 150 min/wk of regular moderate-intensity exercise in their out-patient clinics. Patients were informed of adverse effects of exenatide including dizziness, headache, anorexia, nausea, vomiting, or symptoms of pancreatitis and monitored by physicians. The patients returned at 1, 3, and 6 months for follow-up.
Measurement of the anthropometric and biochemical parameters
The baseline assessments included measurements of height, weight, blood pressure, and fasting blood glucose (FBG), and HbA1c levels. The weights and the HbA1c levels were measured at each visit.
Height and weight were measured without shoes and with light indoor clothes by trained health-care personnel. Body mass index (BMI) was calculated as weight in kilograms divided by height in meter squared (kg/m2). After a 10-minute rest in the outpatient clinic, systolic and diastolic blood pressures were measured in a sitting position, using an automatic device. Blood was drawn after overnight fasting. FBG levels were measured in serum, using a modified glucose oxidase/peroxidase method (Sekisui Medical Co., Tokyo, Japan). HbA1c levels were measured using a G7 Glycohemoglobin Analyzer (Tosoh Co., Tokyo, Japan).
Statistical analysis
The categorical data are expressed as number and percentage of subjects. The continuous variables are expressed as mean and standard deviation.
The changes in HbA1c level and weight over time were estimated by repeated measures analysis of variance. To obtain the best-fit equation for the relationship between the baseline HbA1c levels and the changes in the HbA1c levels with the treatment, a linear model of regression analysis was used. We then analyzed the data using linear-by-linear association to identify the variables associated with the changes in HbA1c level and weight. Multiple regression analysis was used to determine the independent factors for predicting reductions in HbA1c level and weight.
A P value of less than 0.05 was considered statistically significant. The statistical analyses were performed using SPSS for Windows version 17.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
Study subjects' clinical characteristics
Among the 147 patients given exenatide, 95 were excluded for various reasons (Fig. 1). The final analysis included 52 subjects (25 males, 27 females), which were divided into group 1 (exenatide monotherapy for treatment naive patients, n=9/52), group 2 (addition of exenatide to ongoing OHA treatment, n=12/52), group 3 (substitution of exenatide for one kind of OHA, n=23/52), and group 4 (addition of exenatide and OHAs, n=8/52). Baseline characteristics of the study subjects are summarized in Table 1. Of the 52 patients, 25 patients were male (48%), the mean age was 45.1±10.6 years, the mean diabetes duration was 3.2±3.9 years, the mean BMI was 30.0±4.1 kg/m2, the mean HbA1c was 8.5±1.7%, and the mean FBG was 168.2±55.3 mg/dL. Subjects in group 4 had the highest mean values for HbA1c and FBG, while they had the lowest mean value for age.
Effects of exenatide on HbA1c level and body weight
Fig. 2 and Table 2 show the changes in HbA1c level and weight from the baseline to after a 6-month exenatide treatment. Exenatide treatment led to significant improvements in HbA1c in each group: the reductions of HbA1c were 3.1±2.3% (P=0.003) in group 1, 1.3±1.2% (P=0.004) in group 2, 0.8±0.9% (P<0.001) in group 3, 3.5±2.3% (P=0.004) in group 4, and 1.7±1.9% (P<0.001) overall. Weight changes had similar patterns to those of HbA1c. However, group 4 didn't have significant differences in weight between measurements taken at baseline and after the 6-month treatment. The reductions of weight were 8.9±6.7 kg (P=0.004) in group 1, 2.7±2.7 kg (P=0.005) in group 2, 2.7±4.2 kg (P=0.005) in group 3, 2.0±3.6 kg (P=0.159) in group 4, and 3.7±4.9 kg (P<0.001) overall.
Factors affecting the response in HbA1c and weight
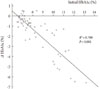
The patients who had higher baseline HbA1c levels had greater reductions in HbA1c level after the exenatide treatment, as indicated by the linear model of the regression analysis (β=-0.896, P<0.001) (Fig. 3).
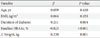
A multiple regression analysis was performed to evaluate the independent factors that might predict HbA1c changes (R2=0.807, P<0.001) (Table 3). Shorter duration of diabetes (P=0.004), higher baseline HbA1c level (P<0.001), and greater reduction in body weight (P=0.001) were the clinical variables that independently suggested greater decreases in HbA1c level with the 6-month exenatide injection therapy. Age and BMI were insignificant factors. On the other hand, the weight changes had no statistically significant relationships with the other variables such as age, BMI, and diabetes duration (R2=0.011, P=0.911) (Table 3).
Safety and tolerability
There were no serious adverse effects related to the exenatide treatment (Table 4). Among the 143 Korean patients who used exenatide, 23 patients (16.1%) had nausea, 17 patients (11.9%) suffered from vomiting, 3 patients (2.1%) complained of dizziness, and 2 patients (1.4%) had erythema on the injection site. Among the 70 patients with T2DM and HbA1c ≥6.5%, who had not used insulin for previous 3 months and did not change more than 2 kinds of OHAs when exenatide was started, 8 patients (11.4%) stopped taking exenatide by themselves due to anorexia or vomiting. Among the 52 study subjects, 8 (15.4%) also had mild nausea, but their symptoms attenuated over time. Neither hypoglycemic events nor the occurrence of pancreatitis was reported during the 6-month treatment.
DISCUSSION
The objective of this study was to investigate the effects of exenatide on HbA1c levels and weight in Korean patients with diabetes. To date, the effectiveness of exenatide in Korean T2DM patients has not been evaluated in real clinical practice.
The present study shows that exenatide therapy reduced the average HbA1c levels and weights by 1.7% and 3.7 kg, respectively. Depending on the prescription regimen, the decreases ranged 0.8% to 3.5% and 2.0 to 8.9 kg. Group 4, the group that started both exenatide and OHAs, had the greatest reduction in HbA1c and group 1, the exenatide monotherapy group, had the greatest reduction in body weight. All four groups showed similar patterns in HbA1c changes. Weight change seemed to follow the trend of HbA1c changes. However, group 4 had insignificant changes between measurements at baseline and after the 6-month treatment, which is assumed to come from the small sample size. There are earlier randomized controlled trials that show the efficacy of exenatide treatment either as a monotherapy or combined therapy with OHAs including metformin, sulfonylurea, and thiazolidinedione. Drucker proved that 10-µg injections of exenatide administered twice daily for 30 weeks resulted in reductions of approximately 1.5% in HbA1c level and 3.6 kg in weight in DURATION-1 study [12]. Blevins et al. [13] documented that a 24-week exenatide treatment reduced HbA1c and weight by 0.9% and 1.4 kg, respectively.
Baseline HbA1c, the duration of diabetes, and weight changes are important confounders to analyze changes in HbA1c. Baseline HbA1c had a negative linear relationship with changes in HbA1c after exenatide treatment. These results correspond well with those found in a recent meta-analysis, which reported that the effect of incretin-based therapy on reduction in HbA1c depended on initial values [14]. Patients with shorter diabetes durations had greater decreases in HbA1c. Those with shorter diabetes durations would have higher possibilities of maintaining the number and function of pancreatic β-cells. It is already a well-known fact that the function of insulin-secreting β-cells is already halved at the time of diagnosis and continues declining thereafter [15,16]. Therefore, some experts insist that early intervention should be started to attenuate this change. There are some laboratory experiments that report exenatide-induced β-cell proliferation, possible neogenesis, and reduced apoptosis [17-19]. The degree of weight loss had clear correlation with changes in HbA1c levels. One possible hypothesis is that weight loss can induce greater HbA1c reductions. Improving insulin resistance through weight loss can have a synergic effect on HbA1c changes by amplifying the function of insulin. However, we cannot confirm if the weight loss actually caused the greater HbA1c reduction or if it was just an independent finding due to decreased food intake. Unfortunately, we had no data to assess β-cell function, insulin resistance, or caloric intake. The results of the multiple regression analysis showed that age and BMI are insignificant variables for HbA1c changes. However, it might be unreasonable to conclude that age and BMI do not affect it since most patients in this study were young and obese.
In contrast to HbA1c levels, weight change had no correlation with other factors. Previous studies have also shown no correlation between baseline body weight and change in body weight [14]. Interpreting the changes in body weight, we must consider lifestyle a confounding factor. It is possible that greater lifestyle modification induces greater weight reduction. Even though all the patients were recommended healthy lifestyle changes, their responses could have been variable.
This study has some limitations. First, there was no control group. Therefore, we cannot estimate the effects of other factors like lifestyle modification. The act of injecting exenatide may have reminded patients to control their lifestyle, including eating a healthy diet and exercising daily. In other trials, the control group that received placebo injections also had a weight reduction, even though the study group that received exenatide injections had a more prominent reduction [20,21]. Second, it is especially difficult to determine whether the effect on HbA1c and weight came from the direct or indirect effects of exenatide because we cannot calculate its effects on hormonal changes such as insulin and glucagon or the subjects' food intake. Neither insulin nor C-peptide was measured before and after the 6-month treatment. In addition, whether patients followed the medical nutrition therapy and exercise recommendation was not evaluated in a standardized manner. Third, the sample size is small and most of the patients in the current study were young and obese. The mean age and BMI were 45.1 years and 30.0 kg/m2. Therefore, we suggest that future studies monitor subjects with a wide range of age and BMI to provide a more accurate evaluation.
Exenatide-induced improvements in glucose level and body weight are expected to bring long-term advantages. However, there is some concern that the use of exenatide might increase the risk of pancreatitis, thyroid cancer, or unexpected adverse effects [22]. Future studies are needed to evaluate the long-term effects of exenatide.
To our knowledge, this is the first study to report the effectiveness of exenatide in a clinical setting. The 6-month exenatide therapy demonstrated significant improvements in HbA1c level and body weight without displaying serious adverse effects in Korean patients with T2DM.





 XML Download
XML Download