

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
There has been an increase in obesity among children and adolescents in all countries of the industrialized world [1]. As with adults, children and adolescents who are overweight or obese face a substantial increase in life-style associated diseases such as type 2 diabetes [2], dyslipidemia [3], hypertension [4], coronary heart disease [5], and stroke [6]. Type 2 diabetes, although still uncommon in children and adolescents in most countries, has nevertheless increased dramatically in recent years, rising from 4% of all pediatric diabetic cases in 1990 to approximately 20% a decade later in the United States [7]. Although clinical implications of atherosclerosis such as coronary heart disease and stroke usually occur in adults, recent studies have demonstrated that obese children and adolescents already show altered lipid profiles and high blood pressure [8]. In addition, autopsy studies have shown that the atherosclerotic process in the vascular wall begins in childhood, especially in the presence of obesity [9].
The measurement of carotid intima media thickness (IMT) of the common carotid artery is an acknowledged noninvasive marker for early atherosclerosis [10]. IMT measurements are feasible, reliable, valid, and cost effective. Carotid artery IMT as a marker of early atherosclerosis has been studied using vascular ultrasonography in children with type 1 diabetes, hypertension, and childhood obesity. Thakore et al. [11] conducted the Framingham Heart Study (n=2,885; 53% female; mean age, 59 years) and reported that inflammatory markers such as C-reactive protein (CRP), interleukin (IL)-6, MCP-1, P-selectin, and CD40 ligand are positively associated with carotid IMT. In addition, Reinehr et al. [12] found that IMT was significantly correlated with body mass index (BMI), body fat, systolic blood pressure (SBP) and CRP among 96 obese and 25 non-obese, healthy, Caucasian, 11-year-old children. These studies suggest that obesity increases levels of inflammatory markers which may cause insulin resistance and in turn, increased carotid IMT.
In addition to inflammatory markers, the insulin-like growth factor (IGF)-1 axis plays an important role in regulation of the structure and function of the cardiovascular system [13]. IGF-1 stimulates vascular cell proliferation and migration from the media into the intima, a step in the progression of atherosclerotic plaque formation [13]. The cellular response to IGFs depends on IGF binding proteins (IGFBPs). Out of six binding proteins identified so far, IGFBP-3 is the protein most often bound to circulating IGF (>80% in adult serum) [14]. Interestingly, both patients with growth hormone (GH) excess and those with GH deficiency have an increased risk of developing cardiovascular events [15]. Furthermore, an increase in IGF-1 and IGFBP-3 has led to conflicting results, in some studies increasing and in some decreasing the risk of developing cardiovascular disease [16-18]. However, there have been limited studies examining the relationship between obesity, fitness, inflammatory markers, IGF-1, IGFBP-3, IMT, and lipid profiles among adolescents.
The purpose of the current study was to investigate the association between obesity, fitness levels, and cardiovascular risk factors and to identify the correlates of IGF-1, IGFBP-3, and IMT among Korean adolescents.
METHODS
Subjects
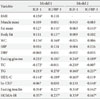
This study was a part of three year longitudinal Korean Adolescents Physical Activity and Health (KAPHA) study. The purpose of the KAPHA study was to investigate the effects of obesity, physical activity participation and physical fitness levels on insulin resistance and cardiovascular disease risk factors among Korean adolescents. The 2nd year KAPHA study has been published [19]. For the current study, data from the first year of the KAPHA study was used. Two hundred twenty five Korean males aged 16.96±0.23 years (BMI, 21.66±3.36 kg/m2) were recruited from a high school in Suwon City, Gyeonggi Province, Korea. The subject characteristics are summarized in Table 1. This study was approved by an Institutional Ethics Review Board at Yonsei University College of Medicine. All subjects gave their written informed consent to participate.
Body weight was measured to the nearest 0.1 kg and height was measured to the nearest millimeter using JENIX DS-102 (Jenix, Seoul, Korea). Waist circumference (WC) and hip circumference (HC) were obtained in duplicate with a Gullick II tape. Percent body fat and total body fat mass were measured by the Inbody 4.0 (Biospace, Seoul, Korea).
Fitness measurement
All fitness measurements were performed by a physical education teacher and exercise physiologist. Musculoskeletal fitness was based on the number of push-ups a student was able to perform [20]. Subjects were asked to put their feet together with 30 cm distance between hands. When subjects were able to lower themselves until their arms were at a 90° angle and then push their body back up to the initial position, it was counted as one successful push-up. The maximum number of push-ups subjects were able to perform were recorded.
Cardiopulmonary fitness was determined by a one-mile run test [21]. Based on data collected during the test, maximal oxygen consumption (VO2max) was estimated using a formula in Cooper Institute for Aerobic Research, 2nd edition. To establish the reliability of this method, we measured the VO2max (Metamax 3B; Corpex Inc., Liepzing, Germany) of 45 subjects. Acquired VO2max results were compared with estimated VO2max using a formula and significant correlation (r=0.77, P<0.001) was identified.
Biochemical analyses
Biochemical tests were performed on blood samples collected after overnight fasting (>12 hours). Serum levels of fasting glucose, total cholesterol (TC), high density lipoprotein cholesterol (HDL-C), triglyceride (TG) and high sensitivity CRP (hs-CRP) were measured using an ADVIA 1650 Chemistry system (Siemens, Tarrytown, NY, USA). IGF-1 and IGFBP-3 levels were measured by an authorized immunoassay using an Immulite 2000 (Siemens, Los Angeles, CA, USA). The intra- and total-assay coefficients of variation for IGF-1 were 3.1±0.7% and 6.2±1.8%; the intra- and total-assay coefficients of variation for IGFBP-3 were 4.4±0.3% and 6.6±0.8%, respectively. Fasting insulin levels were determined by electrochemiluminescence immunoassay (Roche, Indianapolis, IN, USA). Insulin resistance was estimated by homeostasis model assessment of insulin resistance (HOMA-IR) index [(Insulin (µIU/mL)×Fasting blood glucose (mg/dL)/18)/22.5].
Carotid IMT measurement
Ultrasonography of the common carotid artery (CCA) was conducted bilaterally using high resolution B-mode ultrasonography (LOGIQ9; GE Medical Systems, Milwaukee, WI, USA) with a 10-MHz linear transducer. Computer-assisted acquisition, processing, storage of B-mode images and calculation of IMT were performed with the software Intima Scope (MediaCross, Tokyo, Japan). The software estimated lines for the lumen-intima interface and the media-adventitia interface based on 30-point pixels per 3 mm obtained from the tertiary multiple regression analysis incorporating the least square method. This was designed to achieve increased accuracy and reproducibility with reduced variability for the measurements of IMT. Measurements from the left and right CCAs were made at the far walls of the 20-mm segment distal to the carotid bulbs. Reading and analysis of images were done by a single well-trained physician who was blinded to patient identity. IMT results are reported as both average (six point average) and maximum IMT. The intra-observer coefficient of variance was 2.1%. Ninety-two students out of all of the participants were randomly selected for IMT measurement.
Statistical analysis
Statistical analyses were performed using the SPSS version 13.0 (SPSS Inc., Chicago, IL, USA). Subjects were categorized by BMI into low (1st), middle (2nd), and high (3rd) groups, and mean values of all variables were compared over the tertiles of BMI using one way analysis of variance (ANOVA). Pearson's correlation coefficient and partial correlation analysis were used when appropriate. Pearson's correlation coefficient values were categorized as follows: low correlation (0.2 to 0.4), moderate correlation (0.4 to 0.7), and high correlation (0.7 to 0.9). Values of hs-CRP were not normally distributed and thus were log-transformed and analyzed, with statistical significance set at P values of less than 0.05.
RESULTS
Obesity among adolescents increases insulin resistance and cardiovascular disease risk factors
To investigate the relationship between obesity, insulin resistance and cardiovascular disease risk factors, subjects were divided into three groups according to their BMI (tertiles). The mean BMI for each group was 18.41±1.07, 21.22±0.80, and 25.45±2.73 kg/m2, from the least to most obese group. Fasting insulin and HOMA-IR levels were higher in the most obese group compared to the least obese group (Table 2). Factors that represent the degree of obesity such as body weight, fat mass, percent body fat, WC, and waist hip ratio (WHR) were significantly different in each group. HDL-C levels were significantly lower in the most obese group compared to the least obese group.
Relationships between musculoskeletal and cardio-respiratory fitness and metabolic parameters and IMT
To determine the effects of musculoskeletal and cardio-respiratory fitness levels on risk factors for cardiovascular disease and IMT, VO2max values were estimated and the number of push-ups each subject could do was determined. VO2max values were negatively correlated with body weight, BMI, fat mass, percent body fat, WC, TC, TG, fasting insulin, HOMA-IR, IGF-1, and maximum IMT (Table 3). The number of push-ups each subject could do was negatively correlated with body weight, BMI, fat mass, percent body fat, WC, fasting insulin, HOMA-IR, average IMT and maximum IMT (Table 3). After adjusting for BMI, musculoskeletal fitness was still negatively correlated with hs-CRP and maximum IMT; however, VO2max was not significantly correlated with any of the metabolic parameters including IMT levels.
Correlates of growth hormone axis
As presented in Table 4, IGF-1 levels were correlated with body weight, BMI, WC, HC, fasting glucose, TC, TG, HDL-C, fasting insulin, and HOMA-IR. IGFBP-3 levels were also correlated with fat mass, percent body fat, WC, HC, WHR, fasting glucose, TG, HDL-C, fasting insulin and HOMA-IR. After adjusting for BMI, IGF-1 levels were still correlated with fasting glucose, TC, TG, HDL-C, fasting insulin and HOMA-IR. IGFBP-3 levels were also correlated with fat mass, fasting glucose, TG, hs-CRP, fasting insulin and HOMA-IR after adjusting for BMI. IGF-1 and IGFBP-3 both had the strongest correlations with fasting insulin and HOMA-IR levels.
Correlates of IMT
After determining that obesity among adolescents increases cardiovascular disease risk factors, the IMT of 92 of the 225 students was also measured. An IMT six-point average (average IMT) and maximum IMT were used to investigate the correlation between IMT and other variables. The six-point average IMT was significantly associated with weight, BMI, muscle mass, fat mass, and HC (Table 5). In addition, maximum IMT was significantly associated with body weight, BMI, muscle mass, fat mass, percent body fat, WC, SBP, DBP and hs-CRP. However, there was no significant correlation between IMT and IGF-1, nor between IMT and IGFBP-3. After adjusting for BMI, average IMT was not significantly associated with physiological variables; however, maximum IMT was significantly associated with SBP, diastolic blood pressure, and hs-CRP.
DISCUSSION
It has long been known that obesity increases the risk of type 2 diabetes and cardiovascular disease. This study found that adolescent obesity increased insulin resistance, cardiovascular disease risk factors, IGF-1, IGFBP-3, and IMT in the presence of normoglycemia. This study also found that level of fitness was inversely related to obesity, insulin resistance and IMT among Korean adolescent males.
In this study, level of adiposity was not related to fasting glucose levels. Even in the most obese subjects, fasting glucose levels were in the normal range. However, fasting insulin levels increased significantly with adiposity. This suggests that adiposity increased insulin resistance but that increased insulin secretion compensated. It was also recently reported that insulin levels are 125% higher and insulin resistance levels are 77% higher in 26 obese (BMI, 29.5±0.4 kg/m2) adolescents than in 14 lean (BMI, 21.47±0.7 kg/m2) adolescents [22].
Similarly, it was found that IGF-1 and IGFBP-3 levels also increased with adiposity. Increased IGF-1 and IGFBP-3 could be attributed to increased insulin levels in subjects with higher fat mass since insulin promotes the synthesis and biological activity of IGF-1 [23]. In addition to insulin, GH also stimulates the liver to produce IGF-1; indeed, GH is responsible for over 80% of circulating IGF-1 levels [14]. In people with long-term fasting [23] and type 1 diabetes [18], low levels of insulin cause a reduction in hepatic GH receptor levels, resulting in GH resistance and reduced synthesis and levels of IGF-1 in plasma. On the other hand, patients with type 2 diabetes and individuals in over-nourished states, whose endogenous insulin levels and hepatic GH receptors are high, have increased IGF-1 levels [24]. In line with these findings, several cross-sectional studies have reported a positive association between IGF-1 and adiposity [25]. However, these studies found the highest level of IGF-1 only at BMIs between 24 and 27 kg/m2; IGF-1 levels did not increase continuously among subjects with BMIs higher than 27 kg/m2. The results of this study were similar; IGF-1 levels increased with adiposity but IGF-1 levels in subjects with a BMI over 27 kg/m2 were not higher than in subjects with a BMI between 24 and 27 kg/m2.
There is controversy regarding the relationship between IGF-1 and IGFBP-3 and insulin resistance and cardiovascular diseases. Co-administration of recombinant human IGF-1 and IGFBP-3 has shown a dose-dependent reduction of insulin resistance among patients with type 1 diabetes [26]. However, whether higher resting plasma IGF-1 and IGFBP-3 levels positively affect insulin resistance and cardiovascular risk factors still needs to be determined [16-18]. Colao et al. [27] reported that patients with growth hormone deficiency showed abnormal lipid profiles and average IMT compared to normal controls. They also reported that among GH-deficient patients, those with higher IGF-1 levels had better lipid and IMT profiles. Hietaniemi et al. [17] reported that low IGF-1 levels were associated with age, adiposity, TG, insulin and CRP. Based on these previous studies, it appears that high IGF-1 can be beneficial to people with decreased IGF-1 levels such as GH-deficient patients and the elderly.
Another finding of the current study was that IMT increased with adiposity. Increased common carotid artery IMT is significantly related to known cardiovascular disease risk factors and to carotid plaque, a more advanced atherosclerotic lesion [12,28]. Both IGF-1 and IMT increased with adiposity among study subjects; however, unlike in previous studies [17,18], there was no association between IGF-1 and IMT. Most studies that reported a correlation between IGF-1 and IMT were done on adults and elderly patients who had developed relatively severe levels of atherosclerosis [16-18]. However, the average IMT (0.5±0.05 mm) of the subjects in this study was below the level of atherosclerosis diagnosis, so an increase in IGF due to the development of atherosclerosis might have been rare.
Cardiopulmonary fitness was measured to determine the effects of physical fitness on insulin resistance, cardiovascular disease risk factors and degree of obesity. Cardiopulmonary fitness was negatively correlated with the level of adiposity, insulin, insulin resistance, TC, TG, IGF-1, and maximum IMT. However, after adjusting for BMI, the partial correlation analyses showed that the negative correlation between cardiopulmonary fitness and most metabolic parameters was mostly mediated by adiposity. Studies have reported the positive effects of physical activity and cardiovascular fitness on insulin resistance and cardiovascular disease risk factors [29]; some of these studies have been done on children and adolescents [28]. Recently, Hurtig-Wennlof et al. [30] reported that cardiovascular fitness was the strongest predictor for cardiovascular disease. Carnethon et al. [31] investigated data from NHANES on 3,110 adolescents (12 to 19 years) and 2,205 adults, and compared their estimated VO2max with risk factors for type 2 diabetes and cardiovascular disease. They found that in all ages and sexes, BMI, and WC were inversely associated with fitness. Among male adolescents, TC, TG, and SBP levels were higher and HDL-C levels were lower among participants with low fitness than in those with high fitness; the characteristics of these subjects were similar to those of the current study's subjects. Taken together with previous research, it appears that both improvement in fitness and reduction of obesity are important factors for the prevention of cardiovascular disease.
In addition to finding evidence that aerobic fitness helps prevent insulin resistance and metabolic disorders, many exercise intervention studies have demonstrated the beneficial effects of aerobic exercise on insulin resistance and cardiovascular disease risk factors [32]. Recently, it was demonstrated that 6 weeks of jump-roping exercise among obese male Korean youth, which reduced body weight by about 2.5 kg, also significantly reduced insulin resistance and TG and increased adiponectin levels [33]. Meyer et al. [34] also found significant improvements in IMT levels (pre-exercise, 0.48±0.08; post-exercise, 0.44±0.08 mm; P=0.02) after 6 months of exercise training (one hour, three times per week).
Interestingly, not only cardiopulmonary fitness but musculoskeletal fitness was also significantly associated with insulin resistance and average and maximum IMT. Unlike cardiopulmonary fitness, skeletal muscular fitness was still significantly correlated with maximum IMT even after adjusting for BMI, which indicates the importance of musculoskeletal fitness in preventing cardiovascular disease. Although several studies have reported a relationship between cardiopulmonary fitness and cardiovascular disease risk factors and progression of atherosclerosis, this study is the first to show a strong correlation between muscular strength and carotid IMT. Cardiopulmonary fitness has been emphasized over muscular strength to lower cardiovascular disease risk factors. However, recent review articles have stressed the importance of resistance exercise training and subsequent increases in muscle mass for reducing multiple cardiovascular disease risk factors [35]. Further studies are required to determine the effects of resistance training on the risk factors of cardiovascular disease and IMT.
The limitation of the current study is that all participants were male and therefore, these findings may not be applicable to females. In addition, the current study only analyzed cross-sectional data; therefore, it was not possible to determine causality. Another limitation is that the current study did not use a multivariable-adjusted model and did not adjust for other factors such as diet pattern.
In summary, even though there were several limitations such as limited IMT data and homogeneous (males only) participants, this study found that increased insulin resistance, blood lipids, IGF-1, IGFBP-3, and IMT are associated with increased adiposity among male Korean adolescents. In addition, increased fitness levels were associated with decreased insulin resistance and carotid IMT levels, both of which could be mediated by adiposity. Therefore, increased fitness is recommended to not only prevent obesity but also to prevent insulin resistance and cardiovascular disease.




 XML Download
XML Download