

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Most cases of end stage renal disease (ESRD) are caused by diabetes, and the number of cases has increased numerically and proportionally during the last few decades. Diabetic nephropathy, which causes the adverse outcomes of kidney failure, cardiovascular disease and premature death, is now the single most common cause of ESRD in both Western and Eastern countries [1]. However, our ability to assess early renal impairment in diabetic nephropathy, when active management is important, is still poor in comparison to biomarker-based approaches for other diseases, such as serum troponin concentration in acute myocardial infarct [2].
Serum creatinine level is the most commonly used surrogate measurement of glomerular filtration rate (GFR) in a clinical setting. In 2002, the Kidney Disease Outcomes Quality Initiative (K/DOQI) organization published guidelines for chronic kidney disease [3]. This classification, based on the modification of diet in renal disease (MDRD) study estimation equation for GFR using serum creatinine concentration, was immediately widely embraced [4]. However, serum creatinine concentration does not increase until renal function decreases to less than 50% of the normal value [5]. The variances according to age, sex, physical exercise, and lean body mass are also important limitations [6]. Gold standard tests using radioisotopes such as 51Cr-labeled EDTA, 99mTc-labeled DTPA, and 125I-labeled iothalamate or iohexol [7,8] are most reliable for measurement of GFR but are too difficult to use in the clinic setting [9]. Therefore, an accurate and available marker of GFR for patients with diabetic nephropathy is needed.
In the past three decades, urinary albumin excretion has assumed a central role in the diagnosis and management of kidney disease among people with diabetes mellitus [2]. This led investigators during the early 1980s to search for early predictors of diabetic nephropathy through the measurement of low concentrations of albumin in the urine, especially in type 1 diabetic patients [10,11]. Despite a great deal of controversy [4,12], microalbuminuria is now widely accepted as a predictive marker of overt proteinuria [13] and increased cardiovascular disease and mortality [14] not only in type 1 diabetes mellitus [15], but also in type 2 diabetic mellitus [13]. The importance of albuminuria has increased in practice as well as in laboratory research.
However, urinary albumin excretion can be affected by several factors including plasma concentrations of atrial natriuretic peptide, arginine vasopressin, angiotensin II, aldosterone and fasting blood glucose, glycated hemoglobin, and mean arterial blood pressure [16] and albumin can be degraded in a manner consistent with the activity of endogenous urinary proteases [17]. Furthermore, the intraindividual variation is as high as 47%. Because of these problems, all results that are initially positive for albuminuria need to be confirmed with a second sample collected on a different day, and in cases of discrepancies between the first and second sample, a third sample is necessary. Despite the convenience of urinary albumin/creatinine ratio (uACR) measurement in random urine samples compared to 24-hour urine collection, it incommodes clinicians who provide primary care to diabetic patients and causes a delay in the recognition and initial treatment for diabetic nephropathy. It is a fundamental problem because its main purpose is the detection of diabetic nephropathy at an early stage. Therefore, while continuing to encourage the use of the K/DOQI classification, which provides a well-established clinical guideline, the diabetology community should eagerly seek other methods to measure or better estimate early kidney damage of diabetic nephropathy, while maintaining the virtue of uACR. Further, changes in urinary albumin excretion are dynamic, whereas changes in GFR are usually progressive. Although increases in urinary albumin excretion generally precede a decline in GFR, some patients follow a non-albuminuric pathway to renal impairment. Therefore, in the assessment of diabetic nephropathy, the roles of albuminuria and GFR are complementary rather than competitive [18].
Recently, cystatin C was introduced as a good marker of early renal function decline [19,20], particularly in diabetic [21] or elderly [22] patients. Cystatin C is being considered as a potential replacement for serum creatinine because it appears to be less affected by muscle mass [23], and most studies have shown that it is more highly correlated with GFR than is serum creatinine [20,24]. Furthermore, there is no interference from metabolites, like bilirubin, ketones, and various drugs like antidiabetic medications [25]. Cystatin C is a non-glycosylated protein belonging to the super family of cysteine protease inhibitors, and it is produced by all nucleated cells at a constant rate [26]. Serum cystatin C fulfills a number of the criteria that would make it a suitable marker of GFR. It can be freely filtered at the glomerular membrane because of a low molecular weight (Mr=13359) [9] and reabsorbed and catabolized by renal tubular cells [27]. Furthermore, its concentration is stable in stored plasma, unlike urinary albumin, probably due to the high concentration of other proteinase inhibitors [28]. Perkins et al. [29] reported longitudinal data demonstrating that the change in 100/cystatin C was more accurately correlated with the change in iothalamate-GFR than with the change in estimated GFR (eGFR) as calculated from serum creatinine.
Some studies have investigated the correlation between albuminuria and serum cystatin C level, but they evaluated serum cystatin C and albuminuria in cross-sectional datasets [30,31]. Therefore, we analyzed the longitudinal correlation between cystatin C and albuminuria in Korean patients with type 2 diabetes mellitus.
METHODS
Subjects
We collected and retrospectively reviewed the medical records of 1,058 subjects with type 2 diabetes mellitus who visited the out-patient department of the Endocrinology and Metabolism Division at Yonsei University, Gangnam Severance Hospital, Seoul, South Korea from March 2006 to March 2010 (Fig. 1). Inclusion criteria were as follows: 1) previously known type 2 diabetic mellitus; 2) more than 3 years of follow-up for serum creatinine, cystatin C, and uACR; and 3) age between 18 and 85 years. Subjects were excluded if they had 1) significant hepatic disease (alanine aminotransferase or aspartate aminotransferase >2.5-fold the normal value); 2) thyroid disease or medication due to thyroid disease during the previous six months; 3) any other medical condition that could alter the level of serum cystatin C or uACR; or 4) if they were pregnant. The subjects were classified into three groups, according to uACR: 1) normoalbuminuria group (uACR <30 µg/mg); 2) microalbuminuria group (30 µg/mg≤uACR<300 µg/mg); and 3) overt albuminuria group (uACR≥300 µg/mg Cr). Obesity was defined according to 2000 WHO criteria, the Asia-Pacific perspective, as follows; 1) normal weight (body mass index [BMI] <23 kg/m2); 2) overweight (23 kg/m2≤BMI<25 kg/m2); 3) obese (BMI≥25 kg/m2). This study was approved by our human research ethics committee.
Study design
BMI was calculated as body weight in kilograms divided by height in meters squared (kg/m2). Hypertension was defined as systolic blood pressure (SBP) ≥140 mm Hg or diastolic blood pressure (DBP) ≥90 mm Hg and/or reported treatment with antihypertensive medications in the previous 2 weeks. SBP and DBP values were classified by the Joint National Committee (JNC) 7 report in 2003.
Blood was sampled from all of the subjects after fasting for more than 10 hours, and random urine was collected. Serum cystatin C was measured by latex particle-enhanced turbidimetric immunoassays (Cobas 6000 analyzer; Roche Diagnostics, West Sussex, UK). Serum and urine creatinine levels were measured by automatic picric colorimetry (Hitachi 7600-110 automatic analyzer; Hitachi Co., Tokyo, Japan). Hemoglobin A1c (HbA1c) was determined by means of high-performance liquid chromatography (Variant II; Bio-Rad, Hercules, CA, USA). Total cholesterol (TC), triacylglyceride (TG), and high density lipoprotein cholesterol (HDL-C) levels were measured by an enzymatic method using an enzymatic color test (747 automatic analyzer; Hitachi Co., Tokyo, Japan), and low density lipoprotein cholesterol (LDL-C) was calculated according to Friedewald's formula.
The estimated GFR level was calculated using the MDRD formula (MDRD-eGFR) [32]:
MDRD-eGFR=186×(serum creatinine [mg/dL])-1.154×age-0.203×(0.742 if female)
The cystatin C-based estimated GFR (CysC-eGFR) equation [33]:
CysC-eGFR=78/(serum cystatin C in mg/L)+4
To compare the change in variables over three years, we calculated the initial and last value of cysC-eGFR and MDRD-eGFR using two different approaches, as follows:
1) Simple subtraction
2) Declining slope
Statistical analysis
All statistical analyses were performed using SPSS version 18.0 (IBM, Chicago, IL, USA), except for the generalized linear mixed model for longitudinal analysis, which was performed using SAS version 9.0 (SAS Institute Inc., Cary, NC, USA). Serum cystatin C and creatinine concentration were transformed to the reciprocal by multiplying by 100 for analysis. This transformation was performed to assure that changes over time had the same direction as the changes in estimated GFR calculated using the MDRD formula. Descriptive data are expressed as mean±standard deviation, but in the generalized linear mixed model, we used standard error instead of standard deviation. P values less than 0.05 were considered statistically significant.
RESULTS
Clinical and biochemical characteristics of subjects
The clinical characteristics of the study subjects are shown in Table 1. The group of 264 subjects was male-dominant, with an average age of 61.8±10.6 years in the baseline period. The subjects were followed for three years. The proportion of elderly subjects, defined as older than 65 years, constituted almost half of the study group. The mean BMI of these subjects, 24.2±3.0 kg/m2, was in the overweight range, although fewer than 10% of the subjects were obese. Two-thirds of the subjects were prescribed angiotensin-converting enzyme inhibitors and/or angiotension receptor blocker as antihypertensive drugs, and their blood pressures were under control. The mean fasting glucose level of the subjects, 131.1±65.7 mg/dL, was relatively high, but only one-sixth of the patients had an HbA1c greater than 9%, indicating that, overall, the blood sugar levels were under control in this study group.
The mean uACR of subjects was in the microalbuminuria range, and all stages of albuminuria were included. Patients in the nephritic range of proteinuria greater than 2 g/day were excluded because the possibility of other kidney disease could not be eliminated. The portion of patients with renal failure, defined as an eGFR lower than 60 mL/min/1.73 m2, was almost half of the study group. However, if eGFR was calculated using a cystatin C-based equation rather than the MDRD formula, the portion decreased to 34.3%. Patients with end stage renal failure were not included because their status of albuminuria could not be interpreted properly since their urinary albumin was not only glomerular in origin, but also tubular, and some of them had an anuric status.
Longitudinal trends in uACR and renal function marker
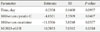
As a result of longitudinal analysis using a general linear mixed model, only 100/cystatin C significantly affected uACR (P=0.0407), while 100/serum creatinine and MDRD-eGFR did not. Serum cystatin C and creatinine values were transformed to the reciprocal multiplied by 100 to assure that changes over time had the same direction as changes in MDRD-eGFR. CysC-eGFR was not involved in this analysis because, unlike MDRD-eGFR, its equation has no other variables except serum cystatin C. uACR decreased to 4.8321 mg/g when 100/cystatin C increased to 1 L/mg (Table 2). Even after adjustment for age, sex, serum uric acid, and HbA1c, these results did not change (P=0.0106); however, the other two renal function markers did not show any effect at all (Table 3). This result was consistent, regardless of the stage of chronic kidney disease stage.
Additionally, age and serum uric acid concentration showed a significant correlation with uACR in serial measurement (P value=0.0023 and 0.027, respectively), although gender and HbA1c did not (P=0.1137, 0.4063, and 0.7372, respectively).
Accordance between uACR and cysC-eGFR or MDRD-eGFR
CysC-eGFR showed better direction accordance (39.4%) with uACR in comparison to MDRD-eGFR (23.8%) (Fig. 2) when analyzing declining slope. When we used the simple subtraction value (Fig. 3), the accordance with uACR increased in both cases (52.3% and 36.8%, respectively), although that of cysC-eGFR was superior. When we categorized the linear variables according to the K/DOQI classification, the accordance rate with uACR was 46.5% in the case of cys-eGFR and 36.1% in the case of MDRD-eGFR. A close look at the discordance portion revealed that cysC-eGFR was worse than MDRD-eGFR at detecting aggravation of albuminuria, and that MDRD-eGFR was worse than cysC-eGFRat detecting improvement in albuminuria or preservation status.
DISCUSSION
In our 3-year follow-up of a hospital cohort of type 2 diabetic patients, neither serum creatinine nor MDRD-eGFR corresponded with the trend in uACR change (Tables 1 and 2). This result indicates that the underlying pathophysiology of albuminuria and GFR loss are different in the early stages of diabetic kidney disease [27], and overt albuminuria does not always precede a significant loss of GFR in the setting of diabetes. Therefore, measuring albuminuria alone does not fully capture the scope of early diabetic kidney disease [10,12]. Instead, albuminuria and GFR loss may represent complementary, if overlapping, manifestations of kidney damage [2].
Most recent studies that have assessed serum cystatin C as a measure of GFR have been cross-sectional in nature, but longitudinal studies are needed to further define the potential role of cystatin C in clinical care [29]. Serum cystatin C has great advantages compared to inconvenient uACR measurements, as mentioned above. Furthermore, there is evidence that cysC-eGFR is more valuable than MDRD-eGFR in the prediction of microalbuminuric stage in a cross-sectional clinical study of Korean type 2 diabetic patients [31]. To our knowledge, this is the first study to suggest a correlation between serum cystatin C and uACR in longitudinal studies for Korean type 2 diabetic patients. In contrast to serum creatinine and MDRD-eGFR, 100/serum cystatin C showed a statistically significant correlation with the trend of albuminuria (estimate -4.8321±2.2339, P=0.0407) (Table 2). Rather, the effect of 100/serum cystatin C on albuminuria increased after adjustments for age, sex, serum uric acid concentration and glycated hemoglobin (estimate -7.6667±2.8110, P=0.0106). However, the effects of 100/serum creatinine (P=0.3857) and MDRD-eGRF (P=0.7229) on uACR remained insignificant (Table 3).
In our study, we demonstrated the superiority of cysC-eGFR in reflecting the trend of albuminuria. But, the discordance portion was nearly half of all subjects (Table 4), so serum cystatin C alone might have limited value as a replacement for uACR measurement.
There are some controversies about the usefulness of serum cystatin C. Many studies have shown that serum cystatin C is a better predictor of cardiovascular disease, renal function [31] and mortality than is the serum creatinine-based eGFR formula [34], although some researchers disagree with this conclusion [21]. The discordance comes from the difference in subject characteristics, mostly with regard to the mean age of the population or proportion of renal failure patients. Our study population was evenly distributed in terms of age and chronic kidney disease stage, thus reinforcing the reliability of our data. It is critical that the ideal marker of diabetic nephropathy not be limited to a certain stage of kidney disease or specific age group because diabetic nephropathy progresses throughout the entire life of diabetic patients and has a broad spectrum from incipient nephropathy to end stage renal disease, which requires dialysis.
The limitations of our study are its retrospective design, the relatively small number of subjects and the fact that the data were collected from a single institute. Additional well-designed, prospective, and multicenter studies with a large population are required in the future.






 XML Download
XML Download