

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The current global prevalence of diabetes in adult population has been estimated to be 5.1% since 2003 and is expected to increase to approximately 6.3% by 2025 [1]. Diabetes is a major risk factor for leading causes of death such as cardiovascular and cerebrovascular disease and is accompanied by multiple complications, which have a negative effect on the family and society. Additionally, as the cost of treating diabetes and its complications have increased continuously, countries have made extensive efforts in preventing and managing diabetes [2].
In most cases, complete recovery after the onset of diabetes is difficult; thus, it is a chronic disease that requires continuous, lifelong therapy and self-management. In addition, several large-scale studies have proven that strict glycemic control and management of comorbidity such as hypertension, dyslipidemia can reduce the occurrence of diabetes complication and mortality rate [3-5]. Therefore, it is recommended that patients start diabetic medication in conjunction with therapeutic lifestyle modification as soon as possible. As known in the previous studies, it is more effective to motivate and educate patients so that they can understand the disease itself and manage their blood glucose level, instead of simply providing medication [6-8]. Enhancing effective self-management skill is an important part of diabetes management, thus, diabetes education is necessary and required as the basis for diabetes care.
The Study Group on Diabetes Mellitus of the World Health Organization (WHO) stated that "The foundation of diabetes management is educating patients and their families on the subject." The American Diabetes Association's mission statement of education program is "Education is an ongoing process with the ultimate goal of a positive behavioral change." Diabetes education is greatly beneficial in patients and furthermore, provides social and economic benefits to society as a whole [9]. In other words, the most effective solution in terms of preventing and controlling chronic diabetic complication is patients' active participation in diabetes management, both of which can be possibly achieved through ongoing patient education and training [10,11]. However, it is difficult to expect effectiveness of the most diabetic education program with one or two sessions conducted in this country [12].
Recently, various individual or group education programs for patients have been offered in several hospitals, and have shown improvement in HbA1c levels, self-management indicators, patient satisfaction and knowledge, shortening of hospitalization period, and reduction in leg amputation rates after the application of these education programs [13,14]. However, the majority of these studies assessed the short-term effects of education on glucose control but not long-term effects after education. In this study, we compared two programs between the existing education program of unilateral information delivery versus intensive, interactive education program for small number of patients, regarding their effects on short- and long-term improvement of diabetes maintenance indicators.
METHODS
Study population
This study is conducted on the patients who were not able to achieve target HbA1c level according to the treatment guideline for diabetes from Korean Diabetes Association [15] (with HbA1c levels ranging 6.5% to 9.0%) and who could be followed for over one year. Patients were devided into two groups based on the education methods. A total of 101 patients had received conventional group education between April 2006 and November 2006, and 106 patients had received a new type of small-group education between December 2006 and July 2007.
Measurement of covariates
We collected patient characteristics such as gender, age, height, weight, duration of diabetes, and history of oral hypoglycemic agents, anti-hyperlipidemic agents, or antihypertensive drugs, or insulin therapy.
We measured the fasting plasma glucose, 2-hour postprandial glucose, HbA1c, total cholesterol, triglycerides, high density lipoprotein cholesterol (HDL-C) and low density lipoprotein cholesterol (LDL-C), and blood pressure at baseline and 3, 6, and 12 months after education. During education, the proportion of patients achieving targeted treatment goals was estimated by examining medical records. The medical records were reviewed retrospectively.
Diabetes education methods
The two types of teaching methods are as follows.
Conventional education (CE)
Approximately 30 in-patients and out-patients were included and group education was offered in two ways: diabetes education executed by a doctor, and diabetes management executed by a nurse for one and half hours followed by a one-on-one nutritional session.
Interactive education (IE)
IE was consisted of approximately 10 people. A nurse, a dietitian, and a physical therapist composed an education team and offered 2.5-hour education sessions. Endocrine specialists were responsible for the entire education system including prescribing medicines and encouraging staffs. Nurses provided education for the patients to understand and manage diabetes, so patients could get overview of disease and verify examination levels, methods for managing and self-monitoring of blood glucose, management of hypoglycemia, foot maintenance, management for special days, and day-to-day activities so as to maintain their daily lives by themselves. Nutritionists emphasized the importance of diabetes-oriented diets and educated patients on proper diet and clinical exercise specialist thought how to exercise for diabetes. Written education aimed at developing a deeper understanding of the program and complementary education via Q & A were also given. After performing small group education and one-on-one private nutritional education, patients received primary and secondary sought management. Blood glucose examinations (HbA1c, blood lipid levels, and blood pressure measurements) were performed in the outpatient clinic at 3, 6, and 9 months after receiving education. Based on the above examination results, a diabetes management instructional flyer was sent out to those patients. Researchers/educators attempted to generate an interest in diabetes management indicators.
Statistical analysis
The crosstab method was used to estimate the proportion of patients who achieve the goals of diabetes management for both groups. The indicators for diabetes management were comparatively analyzed between the two groups at baseline and 3, 6, and 12 months after education. P value less than 0.05 was considered to be statistically significant. All statistical analyses were conducted using SPSS version 17.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
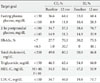
The baseline characteristics of the two groups are shown in Table 1. There were no significant differences between two groups in sex, age, duration of diabetes, the rate of using insulin, oral hypoglycemic or antihypertensive agents. A greater percentage of patients in the IE group reported anti-hyperlipidemic agents use (P<0.001) (Table 1). The mean age of the CE group and IE group was 56.5±12.1, and 55.5±10.6, respectively. The mean duration of diabetes for the CE group and IE group was 5.03±2.3, and 5.1±2.6, respectively and they were not significantly different.
Improvements of management indicators from educational methods
Analytical results of diabetes management indicators in the CE group and the IE group at baseline and 12 months after education are shown in Table 2. Over the 1-year follow up period, the fasting plasma glucose levels significantly dropped from 144.2±30.2 mg/dL to 122.8±19.2 mg/dL in the CE group and from 158.7±49.5 mg/dL to 129.2±25 mg/dL in the IE group, significantly. Comparing two groups, the IE group showed a significantly greater improvement over the CE group (P=0.040). The 2-hour postprandial glucose level for both the CE group and the IE group decreased significantly from 219.8±74.5 mg/dL at baseline to 175.6±48.8 mg/dL and from 212.1±71.6 mg/dL to 159.3±42.1 mg/dL, respectively, one year after education received. Comparing drops of 2-hour postprandial glucose levels between the two groups showed that the IE group had a significantly greater improvement than the CE group (P=0.013).
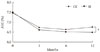
The HbA1c levels of the CE group decreased significantly from 7.5±0.7% to 6.7±0.8% and 6.6±0.6%, 3 and 6 months after education, respectively. However, after 12 months, the HbA1c levels were slightly increased to 6.8±0.6%. The HbA1c levels of the IE group showed a steady decrease, from 7.5±0.8% at baseline to 6.6±0.7%, 6.5±0.8%, and 6.5±0.5% at 3, 6, and 12 months after education received, respectively. The IE group showed greater improvement compared to the CE group (P<0.001) (Fig. 1).
The lipid concentration between the two groups showed no significant differences for HDL-C and triglycerides. However, total cholesterol prior to education were similar as 199.5±37.8 mg/dL and 198.4±41.2 mg/dL, respectively, whereas total cholesterol levels at 12 months after education were significantly different between two groups (168.5±34.7 mg/dL for CE and 157.1±38.2 mg/dL for IE; P=0.026). The LDL-C concentration in the CE group prior to education was 113.3±30.8 mg/dL and 102.9±31.7 mg/dL at 12 months after education. The LDL concentration in the IE group prior to education was 123.1±32.0 mg/dL and decreased to 85.6±28.0 mg/dL one year after education. After one year, there was a significant difference in LDL-C levels between the two groups (P<0.001). The percentage of patients in the IE group taking cholesterol medication was significantly higher than that in the CE group. Although there was a significant decreasing trend in blood pressure for both groups, there was no significant difference between the groups.
Achievement of target goals
According to the American Diabetes Association [16] and the International Diabetes Federation [17] criteria, the primary and secondary (final) target goals were defined and the proportion of patients achieving diabetes management goals are shown in Table 3. One year after education, the proportion of patients that achieve primarily targeted fasting plasma glucose level was increasing in both groups, but there was no significant difference between groups. For the secondary target level, the proportion of patients who achieved target goal was 11.9% for the CE group and was more than doubled to 28.3% for IE group in fasting plasma glucose level one year after education. The proportion of patients who reached the target 2-hour postprandial glucose levels in the primary maintenance goal showed increasing trends in both groups one year after education. For the secondary maintenance goal, 31.3% of patients in the CE group and 35.9% of patients in IE group reached the target one year after education (Fig. 2). The proportion of patients with HbA1c levels below the targeted primary maintenance goal (<7.0%) increased in both groups one year after education. The percentage of patients achieving the secondary maintenance goal in the CE group was 30.7%. The percentage in the IE group was 48.1%, which is significantly higher than that for the CE group (Fig. 3). The proportion of patient achieving the goal of blood lipid concentration increased significantly in both groups one year after education.
DISCUSSION
In the previous study, it has been demonstrated that the effects of diabetes education was favorable on compliance with medications, exercise programs, regular checkups, as well as on significant decreases in 2-hour postprandial glucose levels [18]. However, these promising results were produced using effective education and studies showing the long-term effects of education were limited. The current diabetes education conducted in the most hospitals is being implemented to inpatients, outpatients, and guardians, using instructor-led training for a large group of patients regardless of their different educational levels. Although this education system help increase patients' knowledge about the disease, simple knowledge transmission is insufficient to motivate them. Because this education system is not personalized, even after patients received education, they have difficulties in practicing guidelines for diabetes management and has been failing to reach the target glycemic goal and, therefore, to prevent diabetes complications [19,20]. Thus, developing new educational programs is required.
In this study, we attempted to make changes to the traditional teaching system, to configure a new training program and to evaluate improvements of diabetes management indicators after applying these new educational methods. Although we could not find significant short-term effects of IE (3 and 6 months after receiving education), we identified long-term improvements (12 months after receiving education) on fasting plasma glucose, 2-hour postprandial glucose, HbA1c levels, total cholesterol, and LDL-C.
It is considered to be important education factor to check patients' own laboratory results (e.g., blood glucose, HbA1c levels, and lipid levels) in the result table provided for IE group, and to recognize the differences between targeted goals and their own levels. Additionally, sending out the result tables at 3, 6, and 9 months after receiving education gives the meaning of re-education; recognizing the need for continuous management.
At 3 and 6 months after receiving education, HbA1c levels for both groups showed the decreasing trends. However, after 12 months, HbA1c levels in the CE group showed an increasing trend, while the IE group continued to show a decreasing trend. Thus, for the improvement of long-term maintenance indicators, intervention with sustained, intensive diabetes education is considered necessary.
Although the proportion of patients who achieved their goal of HbA1c <7.0% were similar between two groups, more patients in IE group achieved their targeted goal of HbA1c <6.5%, as result of strict blood glucose control, than those in CE group (48.1% and 30.7%, respectively). In other words, this new education method yielded significant improvements in strict and long-term glycemic control.
Diabetes education in Korea is currently taking place in clinics and public health centers. The insurance policies and fees for health care service are unrealistic, so forming a dedicated education unit and developing a qualified education program are difficult. Most provide perfunctory and one-time education with one-way communication, and it does not guarantee effectiveness of education.
The weaknesses of this study are: 1) it was retrospective study using the medical records of patients; 2) comparison of the degrees of fulfillment of self-management between both groups and changes in the treatment regimen were not investigated one year after receiving education; 3) including only patients who completed the one year follow-up limited generalization of our study findings. Based on this study, a long-term follow-up survey could be planned to determine the prolonged effects of this intensive education program and to evaluate self-management. Furthermore, experiences in diabetes educators and the effects of this education can be shared and this education can be used as a basic material in developing new educational programs in the future.




 XML Download
XML Download