

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Diabetes is an increasing global health problem [1]. The increased prevalence is likely attributable to rapid economic development, improved living standards, an aging population, and a Westernized lifestyle. Diabetes and its complications have become a major cause of morbidity and mortality in Korea [2]. Although diabetes-related mortality has recently decreased from 25.1 per 100,000 persons in 2002 to 19.6 per 100,000 persons in 2009, diabetes is still the fifth-leading cause of death in Korea [2]. Diabetic complications such as renal failure, neuropathy, retinopathy, coronary and cerebral artery diseases, and amputations are associated with increased medical costs and reduced life expectancy [3].
PREVALENCE OF DIABETES AND PREDIABETES: A COHORT STUDY
The first epidemiologic study on diabetes was conducted in the rural area of Okku-gun, Chollabuk-do, in 1971 [4]. With the criteria of ≥160 mg/dL for 1-hour glucose and ≥110 mg/dL for 2-hour glucose after a 50 g oral glucose tolerance test (OGTT), the prevalence of diabetes was 0.91% (1.41% of males, 0.42% of females) among the total subjects aged ≥10 years, and 1.5% (2.5% of males, 0.7% of females) among adults aged ≥30 years (Table 1).
In the 1980s, there was a large, healthcare center-based survey on the prevalence of diabetes [5]. After the 50 g OGTT, diabetes was diagnosed with criteria of fasting glucose ≥140 mg/dL and 1-hour glucose ≥200 mg/dL. The prevalence of diabetes among subjects aged ≥10 years was 3.5% (4.2% of males, 2.4% of females). The prevalence of diabetes increased according to age: 2.2%, 0.5%, 0.9%, 3.4%, 7.1%, 10.4%, and 10.7% in the second to eighth decades, respectively. The prevalence of impaired glucose tolerance (IGT) was 8.0%.
In the 1990s, there were many epidemiologic studies on diabetes prevalence. According to the data from the Korea Medical Insurance Corporation (KMIC), which provides insurance to civil servants and private school workers aged 35 to 59, the prevalence of diabetes was defined as a mean fasting blood glucose of ≥126 mg/dL in 1990 to 1992 was 4.7% in men and 1.3% in women [6]. The prevalence of diabetes in the KMIC cohort may be underestimated because OGTTs were not performed and KMIC workers tend to be healthier than the general population.
A well-designed population-based cohort study was first conducted in Yonchon County in 1993 [7]. A total of 2,520 participants underwent a standard 75 g OGTT. The prevalence of diabetes was 7.2%, substantially higher than that in the previous study, and the prevalence of IGT was 8.9%.
Another population-based study was performed in Jungup District in 1997 [8]. Among 1,108 subjects who completed the 75 g OGTT, the prevalence of diabetes and IGT as defined by the World Health Organization (WHO) criteria were 7.1% and 8.5%, respectively, after correction for Segi's standard world population. When the 1997 American Diabetes Association (ADA) criteria were employed, the prevalence of diabetes and IGT increased to 8.5% and 11.1%, respectively.
An epidemiologic study of diabetes in Korean urban communities was performed in Mokdong, Seoul, in 1998 [9]. There was an 8.5% prevalence of diabetes and 7.8% prevalence of impaired glucose regulation (IGR), including IGT and impaired fasting glucose (IFG). The age-adjusted prevalence of diabetes and IGR was 8.4% and 7.1%, respectively. Interestingly, the prevalence of diabetes in the urban area was slightly higher than that in the rural area.
The Korea Center for Disease Control designed a prospective, large-scale, community-based cohort study [10,11]. In a baseline study in 2001 to 2002, the prevalence of diabetes was 12.6%, including 6.0% known diabetes and 6.6% newly diagnosed diabetes. Accordingly, there was a rapid and dramatic increase in diabetes in Korea.
PREVALENCE OF DIABETES AND PREDIABETES: A NATIONAL SURVEY
With increased attention to social welfare in Korea, the Ministry of Health and Welfare conducted a series of Korea National Health and Nutrition Examination Surveys (KNHANES) to examine the general health and nutrition status of Koreans [12].
The prevalence of diabetes among adults aged ≥30 years in 1998, 2001, 2005, and 2007-2009 was 11.1%, 8.9%, 9.1%, and 9.9%, respectively. The proportion of known cases of diabetes drastically increased from 23.2% in 1998 to 41.2% in 2001, 68.0% in 2005 and 72.3% in 2007-2009. The prevalence of IFG also increased from 17.4% in 2005 to 20.4% in 2007-2009 (Table 2).
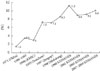
Diabetes and IFG increased dramatically with age in 2007-2009 (Table 3, Fig. 1). Among patients 60 years of age or older, the prevalence of diabetes was estimated to be about 20%, and the prevalence of IFG was about 25%. Diabetes and IFG were more frequent in men than in women.
Therefore, the prevalence of diabetes and IFG in Korea has rapidly increased in the past 40 years from 1.5% to 9.9% for diabetes and 20.4% for IFG (Fig. 2).
INCIDENCE OF DIABETES AND RISK FACTORS
In the 2-year follow-up study on diabetes in the rural area, the annual age-adjusted incidence of diabetes was 3.2% in men and 1.5% in women [13]. Another rural cohort revealed that the age- and sex-adjusted incidence rate of diabetes was 16.3 per 1,000 person-years [14]. The incidence increased as age increased in both sexes. Age, male sex, and fasting and 2-hour glucose levels were significant independent risk factors for the development of diabetes. In the urban area, the age-adjusted annual incidence rate of diabetes for subjects >40 years of age at the baseline was 1.3% [9].
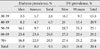
Based on the Task Force Team for Basic Statistical Study of Korean Diabetes Mellitus of the Korean Diabetes Association, the annual incidence of diabetes among Korean adults aged 20 to 79 years was 0.76% (0.73% in men, 0.78% in women) in 2003 [15]. The incidence of diabetes increased with age, but with little difference between men and women. The incidence of diabetes in the 20 to 44, 45 to 54, 55 to 64, and 65 to 79 age groups was 0.26%, 1.19%, 2.04%, and 1.56% in men and 0.18%, 1.04%, 2.09%, and 2.25% in women, respectively.
A recent community cohort study showed that the annual incidence of type 2 diabetes was 1.33% to 2.35% in the 40s, 1.48% to 3.18% in the 50s, 1.85% to 4.55% in the 60s, and 3.08% to 5% in the 70s [11]. A relatively higher incidence was observed in the urban and male populations compared to the rural and female populations.
According to the follow-up study of women with previous gestational diabetes mellitus (GDM), Korean women with a history of GDM have a 3.5 times greater risk of developing postpartum diabetes than the general population [16]. Approximately 40% of women with previous GDM were expected to develop diabetes within 5 years postpartum.
IFG is the most important risk factor for diabetes. Based on the prospective cohort subjects with IFG, 16.6% of men and 6.5% of women had diabetes during the 4-year follow-up [17]. In addition, 21.2% of men and 15.2% of women developed type 2 diabetes in the obese group. Regular exercise is effective in preventing diabetes in people with IFG.
Smoking is an independent risk factor for diabetes [10,18]. Compared to never-smokers, current smokers had a 1.5- to 1.7-fold increased risk.
Metabolic syndrome, as a clustering of metabolic abnormalities, is also an important risk factor for diabetes. According to the KNHANES cohort, subjects with metabolic syndrome had a 1.3-fold increased risk for diabetes [19].
Short sleep duration (≤5 hour) is significantly associated with a 1.2-fold increase in general and abdominal obesity in Korean adults, and is thus associated with increased diabetes [20].
GLOBAL TREND IN DIABETES AND IGT
The International Diabetes Federation provides comprehensive estimates of the absolute numbers and prevalence of diabetes and IGT globally [21]. The total global prevalence of diabetes and IGT in 2010 was estimated at 6.6% and 7.9%, respectively, and is expected to rise to 7.8% and 8.4%, respectively, in 2030 (Table 4). It is estimated that 285 million and 344 million people worldwide will have diabetes and IGT, respectively, in 2010. By 2030, the number of people with diabetes and IGT is projected to increase to 438 million and 472 million, respectively, of the adult population. The largest increases will take place in the regions dominated by developing economies, such as Southeast Asia and the West Pacific region. The prevalence of diabetes and IGT among Korean adults aged 20 to 79 years in 2010 was estimated at 9.0% and 9.4%, respectively, and is expected to rise to 11.4% and 11.5%, respectively, in 2030. The number of Korean people with diabetes and IGT was 3.3 million and 3.4 million, respectively, in 2010, and is expected to increase to 4.3 million and 4.4 million, respectively, in 2030.
CONCLUSIONS
Despite much evidence that diabetes can be prevented or delayed with lifestyle changes and weight loss or certain medications, the diabetic epidemic continues worldwide. The largest increases will take place in the developing regions, such as the West Pacific region, including Korea. With increasing obesity, especially in childhood, decreased physical activity, and improved longevity, diabetes and prediabetes is expected to dramatically increase more than previously projected.
Public efforts to introduce healthy lifestyle changes and systematic diabetes prevention programs are necessary to reduce the global epidemic of diabetes.




 XML Download
XML Download