

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Type 2 diabetes mellitus is a chronic disease characterized by increased insulin resistance, defective β-cell function, and increased hepatic gluconeogenesis [1]. The proportion of patients with type 2 diabetes has been consistently increasing worldwide, and recent increases are remarkable in Asia, including Korea [2,3]. Because the increasing burden of diabetes causes substantial financial loss resulting from increased health care expenditures [4], type 2 diabetes is not a personal disease, but is an important national public health problem.
For glycemic control, life style interventions with metformin are recommended as an initial treatment regimen in a consensus statement from the American Diabetes Association [5]. And there have been many clinical trials in Western countries on the selection of an optimal oral hypoglycemic agent for initial treatment [6-8]. In Japan, Yamanouchi et al. [9] established that several commonly-used oral hypoglycemic agents were equally effective in newly-diagnosed type 2 diabetic patients. However, the doses of each drug were completely different from the usual prescription dosage in Korea, which makes it hard to translate those data into clinical practice in Korea. Furthermore, there has been no head-to-head comparison in a randomized controlled trial to prove the efficacy and safety of antidiabetic agents for Korean type 2 diabetic patients.
This study was designed to evaluate glycemic control efficacy in Korean drug-naïve type 2 diabetic patients receiving monotherapy with a sulfonylurea (glimepiride), a biguanide (metformin), or a thiazolidinedione (rosiglitazone).
METHODS
Study design
This study, called the Practical Evidence of Antidiabetic Monotherapy Study (PEAM), consisted of a multicenter, randomized, double-blind trial performed in 15 centers in Korea. Between February 2007 and December 2008, 435 patients who had not received previous pharmacologic treatment for type 2 diabetes mellitus were screened and 349 patients were randomized to one of three treatment groups. We assigned 118 patients to the glimepiride group, 114 patients to the metformin group, and 117 patients to the rosiglitazone group (Fig. 1). After a 4-week life style intervention, the study drugs were prescribed to each patient. During the lifestyle intervention period, we provided individualized education to each study subject, according to current, recommended guidelines for medical nutritional treatment [10]. We also recommended that each subject perform at least 150 minutes per week of moderate-intensity aerobic physical activity, provided exercise was not contraindicated [10]. Trained dietitians or diabetic nurse specialists provided the education and made these recommendations; however, we did not later verify whether the subjects had followed these recommendations appropriately.
Participants were examined every 8 weeks for 48 weeks from the start of the randomization period. According to the results of HbA1c (<6.5% or ≥6.5%) and drug tolerability check that was performed at each visit, we performed scheduled up-titration of the study drugs (Table 1A). Fasting plasma glucose levels (FPG), HbA1c concentrations, medication compliance, and a physical examination, including taking vital signs and body weight (BW), were assessed or performed at every visit. To evaluate the study participants' medication compliance indirectly, we checked the number of remaining doses at each visit. The ratio of the remaining number of doses at the present visit to the number of doses prescribed at the previous visit was calculated. Subjects with a ratio greater than 30% were excluded in the outcome analysis, since their compliance rate was presumed to be less than 70%. At the outset of randomization and after 48 weeks, we performed a 75 g oral glucose tolerance test. Anthropometric characteristics, demographic characteristics, electrocardiogram, lipid profiles, complete blood counts (CBC), aspartate aminotransferase (AST), alanine aminotransferase (ALT), blood urea nitrogen (BUN), and creatinine were evaluated. All adverse events were recorded and judged for severity and possible relationship to study medications. The study protocol was approved by the Institutional Review Board at each center and all participants provided written informed consent.
Study participants
Eligible study participants were between the ages of 30 and 65 years, with HbA1c levels ranging from 6.5% to 9.5%. None of the subjects had ever taken an oral hypoglycemic agent. Glucocorticoid users, pregnant women, patients who had clinically significant liver disease (AST, ALT>2.5 x upper normal limit), significant renal disease (serum creatinine>1.5 mg/dL in men,>1.4 mg/dL in women), a history of lactic acidosis, a history of unstable angina or severe angina pectoris, a history of or treatment for congestive heart failure, or contraindications to metformin or sulfonylurea treatment were excluded.
Goal assessment
The primary goal of this study was to determine changes in HbA1c levels from baseline (randomization) to end point. The secondary goals were to determine changes in FPG, body weight, and the numbers of subjects achieving target HbA1c levels (<6.5%).
We evaluated differences in all adverse events for the study populations. Hypoglycemia was defined as the presence of typical adrenergic or neuroglycopenic symptoms and signs, regardless of the data for self-monitoring of blood glucose. Edema was defined when the subjects had any signs of fluid retention upon physical examination, or complained of systemic edema.
At baseline, 24 weeks, and 48 weeks, HbA1c levels were measured using high-performance liquid chromatography and FPG was determined using a hexokinase method in a central laboratory (Samkwang Medical Laboratories, Seoul, Korea). Levels of FPG and HbA1c in the other follow-up visits, and lipid levels, were determined using standard assays in each local laboratory.
Statistical analysis
Originally, we calculated a need to enroll 540 study participants to obtain 80% statistical power at a significance level of P=0.05, assuming a 20% attrition rate in each study group. At the end of the study, the overall attrition rate was 34.9%, with a total of 349 randomized subjects. We used an intention-to-treat analysis method in analyzing our data. The last observation carried forward (LOCF) method was used to fill in missing values at a later point in the study. Using per protocol analysis, we included, 82 subjects in the glimepiride group, 71 subjects in the metformin group, and 74 subjects in the rosiglitazone groups in our analysis (data not shown here).
Results are described as mean±standard deviation or median±interquartile range. For comparisons of data among the three treatment groups, a repeated measured ANOVA test was used. For nonparametric statistical analysis, the Kruskal-Wallis test was used. Wilcoxon's signed rank test was used for comparison of pre- and post-treatment values. For analysis of differences in the frequency of adverse events, the chi-square test and Fisher's exact test were used. Statistical analyses were performed using SAS version 9.1.3 (SAS Institute, Cary, NC, USA). Differences among groups with a P<0.05 were considered statistically significant.
RESULTS
Baseline and follow-up characteristics
The subjects' baseline characteristics are described in Table 2. All variables in baseline characteristics were measured at the randomization point. There was no significant difference in HbA1c levels, body weight, blood pressure, and lipid profiles between the screening visit and the randomization visit (data from the screening period not shown here).
The mean age of the total study population was 50.9 years, the mean HbA1c level was 7.8%, and the mean body mass index (BMI) was 25.6 kg/m2. No significant difference was observed in baseline demographics, anthropometrics and metabolic characteristics among the three groups after randomization. Medication compliance was not different in the three groups. The proportion of participants who completed the study was 69.4% in the glimepiride group, 62.3% in the metformin group, and 63.2% in the rosiglitazone group. The number of study participants at each drug dosage level is described in Table 1B.
Primary outcome
HbA1c levels decreased from 7.8% to 6.9% in the glimepiride group (P<0.001), from 7.9% to 7.0% in the metformin group (P<0.001), and from 7.8% to 7.0% (P<0.001) in the rosiglitazone group (Fig. 2). Differences in HbA1c levels from randomization to the end point were -0.89±0.76% in the glimepiride group, -0.92±0.96% in the metformin group, and -0.82±0.79% in the rosiglitazone group. There was no significant difference in the HbA1c levels, or in the changes in HbA1c levels, between the three groups (P=0.62) (Fig. 3A).
Secondary outcome
Levels of FPG decreased from 145.0±32.0 mg/dL to 128.1±27.9 mg/dL in the glimepiride group (P<0.001), from 151.0±32.4 mg/dL to 130.8±25.8 mg/dL in the metformin group (P<0.001), and from 144.1±31.5 mg/dL to 128.6±35.2 mg/dL in the rosiglitazone group (P<0.001). Among the three study groups, levels of FPG at baseline and the end point were statistically different (P=0.52) (Fig. 3B).
Over the study period, significant weight gain was observed in the glimepiride group (ΔBW=1.4 kg, ΔBMI=0.54 kg/m2). In the rosiglitazone group, mean weight increased continuously (ΔBW=1.5 kg, ΔBMI=0.63 kg/m2); however there was significant weight reduction in the metformin group (ΔBW=-1.1 kg, ΔBMI=-0.44 kg/m2) (Fig. 3C).
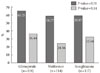
Study participants achieving target HbA1c levels of less than 6.5% were 36.44% (43 subjects) of the 118 members of the glimepiride group, 24.56% (28 subjects) of the 114 members of the metformin group, and 32.48% (38 subjects) in the 117 members of the rosiglitazone group, without significant differences among the three groups (P=0.14). Those with HbA1c level less than 7.0% were 65.25% (77 subjects) of the glimepiride group, 58.77% (67 subjects) of the metformin group, and 58.97% (69 subjects) of the rosiglitazone group, with no significant differences among the three groups (P=0.51) (Fig. 4).
Adverse events
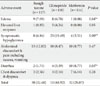
Symptomatic hypoglycemia was more frequent in the glimepiride group (19.49% in glimepiride group vs. 3.51% in metformin group and 6.84% in rosiglitazone group). Diarrhea was more frequent in the metformin group (3.39% of glimepiride group vs. 8.77% of metformin group and 1.71% of rosiglitazone group). Subjective edema as reported by study participants was more frequent in the glimepiride and rosiglitazone groups compared to the metformin group (6.78% of glimepiride group vs. 0.88% of metformin group and 7.69% of rosiglitazone group) (Table 3). Other adverse events, including abdominal discomfort, elevated liver enzymes and chest discomfort or dyspnea were not different in the three study populations.
DISCUSSION
The three study drugs similarly decreased HbA1c levels by 0.8-0.9% by the end of the study. In many previous placebo-controlled trials, glimepiride, metformin, and rosiglitazone lowered HbA1c levels by about 1.0-1.5% [11-13]. The differences between our results and previous studies might be influenced by baseline HbA1c levels, BMI, and prescribed doses of the study drugs. Previous reports in western countries noted participant baseline HbA1c levels 8.5-10% and BMIs of 26-30 kg/m2 [12,13], whereas our study participants had HbA1c levels and BMIs of 7.8% and 25 kg/m2, respectively. We infer these different results may be due to our study population having relatively mild hyperglycemia and lower BMIs.
At the end of the study, the attrition rate was higher than expected (34.9% vs. 20.0%). Therefore, the reliability of our trial was lower than originally estimated at the point of study design.
The fastest response of HbA1c and FPG to the study drugs was observed in study participants receiving glimepiride in the first 24 weeks. This slower action in reducing blood glucose levels using metformin and rosiglitazone, as compared to glimepiride, is similar to a previous report [14]. The maximum hypoglycemic effect was seen at 32 weeks in the glimepiride and rosiglitazone groups and at 40 weeks in the metformin group; therefore, an observational period at least 6 to 8 months appears to be needed to judge whether a patient is responding to a specific oral antihyperglycemic drug.
Although about 60% of the study participants reached a target HbA1c level of less than 7.0%, the rest of the study participants remained in an inadequate glycemic control state. And only about 30% of the subjects reached a target HbA1c less than 6.5%. To improve the state of patients' glycemic control, more active treatment should be performed and additional studies and analyses are needed to elucidate several factors influencing the level of glycemic control.
Whereas metformin does not cause weight gain and may induce modest weight loss in type 2 diabetic patients, glimepiride and rosiglitazone generally result in weight gain [15-17]. In this study, metformin induced significant weight loss, while glimepiride and rosiglitazone induced significant weight gain in Korean type 2 diabetic patients. This suggests a useful and beneficial health effect to using metformin for obese or overweight Korean diabetic patients.
As in previous studies [18], the most common side effect was symptomatic hypoglycemia in the glimepiride group. Although metformin and rosiglitazone are not known to induce hypoglycemia [19,20], a few study participants in those groups complained of hypoglycemic symptoms; however, these complaints cannot be confirmed as true hypoglycemia, as our study did not involve self-monitoring of blood glucose levels at the time the study participants felt hypoglycemic symptoms.
The main adverse event with metformin was diarrhea; with rosiglitazone, it was edema due to fluid retention and weight gain. Overall, 8-12% of study participants experienced abdominal disturbances including pain, discomfort, nausea, or vomiting during the study period; however, the symptoms were transient in the majority of the study participants and the causal relationship between the study drugs and symptoms is uncertain. We did not assess actual changes in lipid parameters during the study due to use of additional anti-hyperlipidemic agents. Lipid parameters are important in understanding secondary effects of the study drugs and are changeable according to the agents used [9,21]. Future studies should be designed to evaluate the true effects of antihyperglycemic agents on lipid parameters in Korean patients.
In conclusion, this study demonstrates that the efficacies of glimepiride, metformin, and rosiglitazone are similar, with no statistical differences, when used for antidiabetic monotherapy in drug-naïve type 2 diabetic patients. This trial is the first randomized controlled trial to evaluate the efficacy of commonly-used antidiabetic agents in Korean type 2 diabetic patients. Specific characteristics of the study drugs should be considered when choosing an appropriate agent. To use these results as valuable information for selecting an oral hypoglycemic agent, more detailed subgroup analyses and further investigation is recommended.





 XML Download
XML Download