

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Metastasis of a primary carcinoma to the adrenal glands is not rare, occurring in 10%–25% of carcinoma cases (12345). With the development of imaging modalities, the incidental detection of adrenal gland lesions at the time of primary tumor diagnosis or during follow-up has increased (67). Adrenal gland metastases commonly occur in patients with lung, kidney, breast, or gastrointestinal carcinomas (6).
Distant metastasis from a carcinoma can be classified as synchronous or metachronous. Synchronous metastasis usually has a poor prognosis owing to the advanced stage of the disease at the time of diagnosis and requires multiple treatment modalities. Metachronous adrenal metastases had favorable outcomes in previous studies, some of which recommended resection as the treatment modality in patients with no evidence of other metastatic lesions (489).
The type of surgical approach used to manage isolated adrenal metastases can affect the surgical outcome. Initially, open adrenalectomy (OA) was the only surgical option. However, since its inception, laparoscopic adrenalectomy (LA) has been used to treat malignant adrenal lesions with acceptable surgical outcomes (61011).
The aim of this study was to determine the post-adrenalectomy oncologic outcomes for isolated metachronous adrenal metastases with no evidence of disease (NED) after treatment of the primary carcinoma and to identify the patients most likely to benefit from metastatic adrenalectomy. Additionally, we compared the outcomes between OA and LA.
METHODS
1. Study population
Seventy-seven patients with isolated metachronous adrenal metastases from solid primary carcinomas underwent metastatic adrenalectomy at the Asan Medical Center, Seoul, Korea from January 2000 to December 2010; these included patients with NED after treatment of the primary carcinoma and before diagnosis of adrenal metastasis. After review of the medical records, patients with synchronous metastasis (n=28), persistent primary carcinomas (n=9), resection-positive margins with tumor remnants (n=3), combined metastasis (n=16), or double primary carcinomas (n=2) or those lacking medical records (n=5) were excluded. Ultimately, 21 patients were included in this study, 5 of whom are still alive.
2. Follow-up protocol
The patients were evaluated via preoperative imaging, including abdominopelvic computed tomography (CT), chest CT, magnetic resonance imaging (MRI), and/or positron emission tomography (PET). Diagnosis of adrenal metastasis was confirmed via CT, MRI, and/or PET during the follow-up period. Routine follow-up exams were performed every 6 to 12 months according to the patient's clinical condition.
3. Prognostic outcomes
For each patient, clinical data (e.g., age, sex, origin of the primary carcinoma, the interval between initial treatment and adrenalectomy, site and size of the metastatic adrenal tumor, overall survival [OS], disease-free interval [DFI], disease-specific recurrence-free survival [RFS], and type of adrenal surgery) were analyzed. OS was defined as the time between primary carcinoma treatment (surgery, n=15; other, n=6) and last follow-up. DFI was defined as the time between primary carcinoma treatment and metastatic adrenalectomy. Disease-specific RFS was defined as the time between metastatic adrenalectomy and the second recurrence after adrenal surgery. Disease-specific RFS times based on the origin of the primary carcinoma, the size of the metastatic adrenal tumor, the date of metastatic adrenalectomy, and the type of adrenal surgery were determined.
4. Statistical analysis
Continuous variables are presented as mean±standard deviation with ranges, and categorical variables are presented as percentages and absolute numbers. To determine the cutoff values for significant continuous variables for clinical application, the area under the curve (AUC) was calculated via receiver-operating characteristic (ROC) curve analysis. Survival outcomes were analyzed using the Kaplan-Meier method and the log-rank test. A P value <0.05 was considered significant. Analyses were performed using SPSS software, version 20.0, for Windows (SPSS Inc., Chicago, IL, USA).
RESULTS
Our study included 21 patients with isolated metachronous adrenal metastases from a primary carcinoma who had NED at the time of metastatic adrenalectomy. Fifteen patients received surgery as the primary carcinoma treatment, and 6 received non-surgical treatment (transcatheter arterial chemoembolization for hepatocellular carcinoma, n=1; combined chemotherapy and radiation therapy for pulmonary carcinoma, n=4) (Table 1). The study cohort included 17 men and 4 women, with a mean age of 54.6 years. Hepatocellular carcinoma was the most common primary carcinoma (n=10, 47.6%) followed by pulmonary carcinoma (n=8, 38.1%) and other carcinomas (n=8, 14.3%). The mean size of the metastatic adrenal tumor was 4.8 cm. The mean OS, DFI, and disease-specific RFS times were 78.5, 23.9, and 34.0 months, respectively. Most patients received OA (n=15, 71.4%); the others received LA (n=7, 28.6%).
Table 1
Clinical characteristics of patients who underwent metastatic adrenalectomy for adrenal metastases from other primary carcinomas after the initial treatment

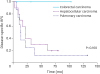
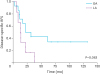
Among the 3 types of primary carcinoma, there was no significant difference in OS (P=0.146) (Fig. 1), DFI (P=0.174), or disease-specific RFS (P=0.160) (Fig. 2). Because there was no difference in OS or disease-specific RFS among these groups, we performed a forwarding analysis of the entire patient cohort. Disease-specific RFS times based on the size of the metastatic adrenal tumor, the date of metastatic adrenalectomy, and types of adrenal surgery were determined. There was no definitive cutoff value for the size of the metastatic adrenal tumor in the ROC analysis (AUC=0.567). The cutoff value for the DFI that was associated with the disease-specific RFS time was 16.5 months (AUC=0.739). A survival curve showed a significant difference between DFIs <16 months vs. ≥16 months (P=0.043) (Fig. 3). There was no significant difference in disease-specific RFS times between OA and LA (P=0.063) (Fig. 4).
Fig. 1
OS rate of all patients after the initial treatment of primary carcinoma.
OS = overall survival.
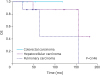
Fig. 2
Disease-specific RFS rate of all patients after the metastatic adrenalectomy.
RFS = recurrence-free survival.

DISCUSSION
In this study, patients with isolated metachronous adrenal gland metastases who underwent adrenalectomy had an acceptable disease-specific RFS duration. This was especially evident in patients in whom metastasis occurred at least 16 months after treatment of the primary carcinoma. All patients had NED (other than adrenal gland metastases) at the time of adrenalectomy.
Several studies have assessed the feasibility of adrenalectomy for adrenal metastases (2461012). However, most of them focused on the outcomes of OA vs. LA. Only a few examined post-adrenalectomy survival times, and the number of cases in these studies was small (134131415). Hence, information about the prognosis of patients after metastatic adrenalectomy is lacking.
Earlier studies evaluated the relationship between the size of the metastatic adrenal lesion and long-term survival. Marangos et al. (2) found no significant difference in survival times for small (<6 cm) vs. large (>6 cm) metastatic adrenal tumors in 41 patients who underwent surgical resection (P=0.840). Tomasini et al. (1) reported that adrenalectomy for adrenal metastases was feasible regardless of their size or origin. Similarly, in our study, the size of the metastatic adrenal tumor did not significantly affect the disease-specific RFS time.
Several studies assessed the use of the DFI as a prognostic factor for postoperative outcomes in patients with adrenal metastases. Solaini et al. (3) showed that a long DFI was a positive prognostic factor, and Howell et al. (16) reported that median survival time was extended when the DFI was ≥12 months compared with <12 months (41 vs. 13 months). In studies by Sarela et al. (12) and Kim et al. (4), a DFI >6 months was the only factor associated with improved survival. Our results also identify the DFI as a prognostic factor for patients with adrenal metastases, especially when the interval between initial treatment and metastasis is ≥16 months. In this instance, the disease-specific RFS time may be increased (P=0.043).
Since its first description by Gagner and colleagues (17) in 1992, LA has become the standard method for management of benign adrenal masses (261017). However, its use for treatment of solitary metastases or primary adrenal carcinomas is controversial owing to the possibility of carcinomatosis or port site metastasis which would worsen the oncological outcome (11). The indications for LA have recently expanded, and surgical removal of metastatic adrenal glands has become more acceptable owing to reports documenting long-term survival after LA (1115). Compared with OA, LA may result in less intraoperative blood loss, shorter hospital stays, and better cosmetic outcomes (12). Although there is controversy, support for LA for treatment of malignancies is increasing as more and more instances of LA use are reported (121518). In our study, there was no significant difference between LA and OA in terms of long-term survival (P=0.063), which suggests that the survival benefits of LA are not inferior to those of OA.
The limitations of this study are as follows. First, the size of the study population was small, which may have introduced selection bias. Second, the general conditions of the patients were not standardized, which may have affected the survival times. Third, this study was retrospective, and we unable to determine why the different types of surgery were chosen.
CONCLUSION
Metastatic adrenalectomy is a treatment option for isolated metachronous adrenal metastases in patients with NED after treatment of the primary carcinoma. Post-adrenalectomy survival was better when the interval between primary carcinoma treatment and metastatic adrenalectomy was ≥16 months. Hence, surgical treatment is recommended for isolated metachronous adrenal metastases in such patients. Additionally, LA was not inferior to OA in this study; however, this result needs to be further tested in a prospective randomized study with a larger patient cohort.
 XML Download
XML Download