

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Papillary thyroid cancer (PTC) is the most common cancer of the thyroid, accounting for more than 90% of all cases in Korea, and the least aggressive form of thyroid cancer (1). Consequently, the debate on the appropriate treatment of patients with PTC has persisted for several decades. Despite favorable disease prognosis, in a subgroup of patients, PTC behaves aggressively and is associated with recurrence and poor survival (23). Therefore, identification of specific disease characteristics associated with prognosis, including accurate staging, has become important in defining the PTC biology and in directing therapeutic intervention.
Lymph node status has been shown to be related with local recurrence, and with disease-specific survival in older patients (456). PTC involves cervical lymph node metastasis in 20%–50% of the patients and metastasis may occur even when the primary tumor is small and intrathyroidal (78). The most common site of nodal metastases is the central neck. In many patients, lymph node metastases in central neck do not appear abnormal on preoperative imaging or during an inspection at the time of surgery and are classified as clinically negative lymph nodes (9101112). Therapeutic lymph node dissection in patients with clinically evident lymph node involvement is a well-established surgical intervention (13). However, the value of routine prophylactic central compartment neck dissection for clinically node negative disease remains controversial. For some prognostic features associated with an increased risk of metastasis and recurrence such as larger tumor size, multifocal disease, extrathyroidal extension, and known lateral node metastases, prophylactic central neck dissection is considered during therapeutic decision-making and disease control (121415).
PTC often presents as multifocal or bilateral tumors, and the incidence of multifocality varies widely in previous studies, ranging from 18% to 87% (161718). Multifocal tumors have been associated with increased risks of lymph node and distant metastases, persistent local disease after initial treatment, and regional recurrence (19). However, few studies have investigated the difference in the impacts of bilaterality and unilateral multifocality on lymph node metastasis in PTC.
The aim of this study was to evaluate the association between cervical lymph node metastasis and disease multifocality, bilaterality, and other clinicopathological features of PTC, in order to assist surgical decision-making. We further evaluated the relationship between the number of PTC foci and the frequency of metastasis to the cervical lymph node.
METHODS
1. Patients
We retrospectively reviewed the medical records of 819 patients who underwent total- or hemithyroidectomy for PTC at the Kyungpook National University Medical Center between January and December 2013. The PTC diagnosis was confirmed pathologically, and the PTC cases with follicular or medullary cancer and focal anaplastic change were excluded. All patients underwent preoperative ultrasound examination for the assessment of the tumor number, tumor location, and central or lateral cervical lymph node metastasis. Ipsilateral central neck dissection was performed for all patients. Patients with clinically proven lateral neck metastasis underwent modified radical neck dissection.
The following data were analyzed in the groups: age at the time of surgery, sex, primary tumor size, tumor extent, tumor foci number, presence of lymph node metastasis, tumor-lymph node-metastasis (TNM) stage, Hashimoto's thyroiditis, and BRAFV600E
mutation status. Tumors were classified based on the standardized TNM system of the American Joint Committee on Cancer (20).
Based on multifocality and bilaterality, the study population was divided into 4 groups: 1) group 1, patients with unilateral solitary PTC; 2) group 2, patients with unilateral multifocal PTC; 3) group 3, patients with bilateral solitary PTC; and 4) group 4, patients with bilateral multifocal PTC. Bilateral PTC was defined as histopathologically diagnosed cancer in both thyroid lobes; occult tumors were also included. Multifocality was defined as 2 or more tumor foci within one lobe of the thyroid. For multifocal tumors, the diameter of the largest tumor focus was recorded as the primary size. We analyzed the differences in clinicopathological features among the above-mentioned groups and assessed the relationship between the number of PTC foci and lymph node metastasis.
2. Statistical analysis
The clinicopathological features among the study groups were compared using the Fisher's exact test and Pearson's χ2 test. A multivariate logistic regression analysis was employed to evaluate the independent effect of the number of PTC foci on cervical lymph node metastasis. All statistical analyses were performed using the Statistical Package for Social Sciences for Windows (SPSS; SPSS Inc., Chicago, IL, USA). A P value <0.05 was considered statistically significant.
RESULTS
1. Baseline characteristics
At the time of diagnosis, the mean age of the 819 study participants was 47.4 years (range 16–80 years; median 47 years), and 703 participants (85.8%) were females. The mean size of the largest tumor focus was 0.96 cm (range 0.2–4.6 cm). An extrathyroidal extension was reported in 401 (50.0%) patients, and the BRAFV600E
mutation rate was 85.8%. Cervical lymph node metastasis on final pathology was noted in 340 patients (41.5%). Central and lateral cervical lymph node metastasis were reported in 339 (41.4%) and 38 (4.6%) patients, respectively, and of them, 1 patient had only lateral cervical lymph node metastasis, without central node metastasis. Multifocal PTC in one or both lobes was reported in 215 patients (26.3%) and 210 patients (25.6%) had bilateral disease (Table 1). Of the patients with multifocal disease, 166 had 2 PTC foci, 108 had 3–4 foci, while 6 patients had ≥8 foci (Table 2).
Table 1
Baseline clinicopathological characteristics of patients with PTC in the study groups


2. Multifocality and bilaterality of PTC
The study participants were segregated into 4 groups based on PTC multifocality and bilaterality: 1) group 1, unilateral solitary PTC (n=511; 62.4%); 2) group 2, unilateral multifocal PTC (n=98; 11.9%); 3) group 3, bilateral solitary PTC (n=93; 11.4%); and 4) group 4, bilateral multifocal PTC (n=117; 14.3%). The patient characteristics in each study group are listed in Table 1. There was a significant difference in the frequency of cervical lymph node metastasis among the 4 groups (P<0.001). The frequency of central and lateral cervical lymph node metastasis was highest in the bilateral multifocal PTC group, followed by the bilateral solitary group, unilateral multifocal group, and the unilateral solitary PTC group. There were also significant differences in the tumor size (P<0.001) and tumor extent (P=0.006) among these groups.
No significant clinicopathological differences were observed between groups 3 and 4. Our data showed similar rates of cervical lymph node metastasis between the 2 bilateral PTC groups. Further, the clinicopathological variables and the frequency of cervical lymph node metastasis did not differ between patients with unilateral solitary PTC and those with unilateral multifocal PTC. The patients with unilateral multifocal PTC had significantly smaller sized tumors (<10 mm), less extrathyroidal extension, and lower rates of cervical lymph node metastasis than the patients with bilateral solitary or multifocal PTC.
3. Number of PTC foci
The effect of the number of PTC foci on cervical lymph node metastasis was further examined (Table 2). The presence of cervical lymph node metastasis was significantly different based on the number of tumor foci (P<0.001), and patients with more tumor foci exhibited lymph node metastasis more frequently compared with those with fewer tumor foci. Of the 511 patients with unilateral solitary PTC, 187 (36.6%) had cervical lymph node metastasis. Similarly, 24/73 (32.9%) patients with unilateral PTC with 2 tumor foci had cervical lymph node metastasis. The proportion of patients with positive cervical lymph nodes increased to 50/93 (53.8%) in patients with bilateral PTC with 2 tumor foci (one focus in each lobe). In comparison to unilateral solitary PTC group, the frequency of cervical lymph node positivity nearly doubled in the group with 5–7 foci, where 20/28 (71.4%) patients exhibited lymph node metastasis. Furthermore, cervical lymph node positivity was observed in all patients with >8 or more PTC foci, 6/6 (100.0%).
4. Risk factors for cervical lymph node metastasis
A univariate analysis demonstrated that cervical lymph node metastasis was significantly associated with the male sex, age <45 years, tumor size ≥10 mm, extrathyroidal extension, advanced TNM stage, and bilateral PTC (Table 3). However, the BRAFV600E
mutation was not associated with lymph node metastasis (P=0.736). In a multivariate analysis, male sex (odds ratio [OR], 1.89; 95% confidence interval [CI], 1.28–2.82; P=0.002); tumor size ≥10 mm (OR, 3.15; 95% CI, 2.31–4.33; P<0.001); minimal extrathyroidal extension (OR, 2.55; 95% CI, 1.92–3.41; P<0.001); invasion to the trachea, esophagus, or recurrent laryngeal nerve (OR, 9.17; 95% CI; 2.26–61.29; P=0.006); and the disease stage III and IV (OR, 3.58; 95% CI, 2.66–4.83; P<0.001) were significantly associated with cervical lymph node metastasis (Table 4). There was no association between unilateral multifocal PTC and cervical lymph node metastasis (OR, 1.00; 95% CI, 0.63–1.55; P=0.992). Bilateral solitary PTC (OR, 2.00; 95% CI, 1.28–3.13; P=0.002) and bilateral multifocal PTC (OR, 2.30; 95% CI, 1.53–3.48; P<0.001) were found to be independent predictors of cervical lymph node metastasis. In addition, the presence of >3 PTC foci was also an independent predictor of metastasis, and as the number of PTC foci increased, the rate of cervical lymph node metastasis increased significantly. In patients with 2 tumor foci, unilateral PTC had no association with lymph node metastasis (OR, 0.84; 95% CI, 0.49–1.40; P=0.516), however, bilateral PTC with 1 tumor focus in each lobe was significantly associated with cervical lymph node metastasis (OR, 2.00; 95% CI, 1.28–3.13; P=0.002). In a multivariate analysis for evaluating the predictors of 5 or more lymph node metastasis, the male sex (OR, 2.41; 95% CI, 1.38–4.10; P=0.002); age <45 years (OR, 1.59; 95% CI, 1.00–2.53; P=0.049); tumor size ≥10 mm (OR, 7.87; 95% CI, 4.77–13.37; P<0.001); minimal extrathyroidal extension (OR, 4.28; 95% CI, 2.50–7.69; P<0.001); invasion to the trachea, esophagus, or recurrent laryngeal nerve (OR, 10.11; 95% CI; 2.05–40.02; P=0.002); and the disease stage III and IV (OR, 1.61; 95% CI, 1.01–2.56; P=0.045) had the significant association (Table 5). Bilateral solitary PTC (OR, 2.35; 95% CI, 1.15–4.57; P=0.014), bilateral multifocal PTC (OR, 4.35; 95% CI, 2.48–7.57; P<0.001), and the presence of >3 PTC foci were independent predictors of 5 or more lymph node metastasis.
Table 3
Univariate analysis of factors associated with cervical lymph node metastasis
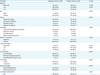
Table 4
Multivariate analysis for predictors of cervical lymph node metastasis

Table 5
Multivariate analysis for predictors of 5 or more cervical lymph node metastasis

DISCUSSION
Multifocality has been reported in 18%–87% of patients with PTC (161718). In this study, the prevalence of multifocality was 37.6%, and that of bilaterality was 25.6%. Our results show that the bilateral PTC significantly increased the risk of cervical lymph node metastasis compared with unilateral multifocal PTC. There was no difference in lymph node metastasis between unilateral solitary PTC and unilateral multifocal PTC. Furthermore, patients with bilateral solitary or multifocal PTC had larger tumors, more extrathyroidal extension, and higher frequency of lymph node metastasis.
Recently, several studies have described multifocality and bilaterality associated with cervical lymph node metastasis in the patients with PTC; however, the findings reported in these studies are not consistent. Wang et al. (21) reported that bilateral PTC is common, occurring at a frequency of 19.9% in their cohort, and that bilaterality is associated with poor prognosis. Increased rates of extrathyroidal extension, nodal metastasis, as well as an overall higher stage at presentation were all associated with bilateral disease. Qu et al. (22) reported bilateral-multifocality as a subtype of PTC and that it was associated with more aggressive features such as larger primary tumor size, more frequent extrathyroidal extension, and cervical lymph node metastasis. Furthermore, they also reported that bilateral-multifocal PTC rather than unilateral multifocal PTC was an independent predictor of poor prognosis. In contrast, Kim et al. (23) reported that although multifocal and bilateral PTC had aggressive pathologic features, only multifocality was an independent predictor of disease recurrence and persistence.
In our study, the risk of cervical lymph node metastasis increased proportionally with the number of tumor foci in patients with >3 PTC foci. There was no appreciable difference in cervical lymph node metastasis between unilateral patients with PTC with one (36.6%) or 2 foci (32.9%). However, bilateral PTC with one focus per lobe was significantly associated with cervical lymph node metastasis (53.8%). In comparison, cervical lymph node positivity doubled in the presence 5–7 foci (71.4%), and tripled in the presence of ≥8 PTC foci (100%). More recently, Al Afif et al. (24) investigated the effect of the number of PTC foci on lymph node metastasis, and reported a trend similar to the one we observed in our study. In their cohort, lymph node metastasis doubled in the presence of 3–9 foci (38%), and quadrupled in the presence of >10 foci (88%), when compared with unifocal (22%) and bifocal (19%) PTC disease. However, they did not find any association between lymph node positivity and PTC bilaterality.
Univariate and multivariate analyses identified metastasis risk factors such as the male sex, age <45 years, tumor size ≥10 mm, extrathyroidal extension, and advanced TNM stage. Previously published studies have also identified these risk factors of cervical lymph node metastasis (242526). Even as bilateral solitary and bilateral multifocal PTC were identified as independent predictors of cervical lymph node metastasis, no association was noted between unilateral multifocal PTC and cervical lymph node metastasis. Moreover, in our study, although both PTC multifocality and bilaterality were associated with aggressive pathological features, bilaterality weighed more than multifocality in predicting cervical lymph node metastasis.
In a multivariate analysis, a higher number (>3) of PTC foci was associated with cervical lymph node metastasis. In patients with 2 PTC foci, a significant increase in lymph node metastasis was observed when the tumor foci were distributed one per lobe (OR, 2.00), while no significant increase was observed when both foci were located in the same lobe. No previous studies have reported an effect of the lobe-wise distribution of tumor foci on metastasis.
The clinical impact of lymph node metastases is strongly dependent on several other features such as the number of metastatic nodes, the size of the metastasis, and the presence of lymph node capsular invasion. The presence of few (<5) metastatic lymph nodes with foci of <2 mm has probably little or no impact on the prognosis of the patient. In this study, the presence of multiple bilateral foci or more than 3 foci are independent risk factors of 5 or more lymph node metastases.
In our study, patients with bilateral PTC and >3 tumor foci had a higher risk of lymph node metastasis at the time of surgery, and total thyroidectomy combined with prophylactic central compartment neck dissection should be considered as the standard surgery for such patients. However, hemithyroidectomy with prophylactic central neck dissection alone is sufficient for the treatment of unilateral multifocal PTC.
This study has its limitations. As a retrospective chart review, this investigation does not shed light on long-term outcome of PTC patients according to the presence or absence of lymph node metastases. And the categorization of tumors as unilateral and bilateral was limited by the presence of patients who had undergone hemithyroidectomy. The number of patients included represents a relatively small cohort in single center. Thus, multicenter research and long-term follow-up are needed to better understand the risk factors and the significance of prophylactic central neck dissection.
In conclusion, there was a significant association between bilateral PTC and lymph node positivity, which increased proportionally with the number of PTC foci. Bilateral solitary or multifocal PTC was associated with more aggressive clinical features such as greater primary tumor size, as well as more frequent extrathyroidal extension and regional lymph node metastasis. In addition, bilateral PTC rather than unilateral multifocal PTC was an indicator of disease aggressiveness, as seen by the increased tendency for metastasis to the regional lymph node.
 XML Download
XML Download