

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Pathological anomalies (i.e. nerve displayed from goiter, nodule, lymph node, scar tissue, or radiation) and anatomical anomalies of the recurrent laryngeal nerve (RLN) can not only mean an operational challenge in thyroid operations for the endocrine surgeon, but also an increased risk of postoperative vocal cord paralysis (VCP) (12).
Atypical courses of the RLN are frequent and observed in about a quarter of the thyroid gland operations (123456789). Anatomical RLN variations are represented by; 1) an atypical RLN pattern as anterior or lateral to the thyroid gland, 2) an anteriorly RLN to a Zuckerkandl tuberculum nodule, 3) a fixed, splayed, or entrapped RLN with capsular association through fascial bands, 4) an invaded RLN, 5) a nerve posterior to ligament of Berry, 6) a thin <1 mm nerve, or antevascular RLN, 7) a non-RLN, and 8) a ramificated RLN (1234). The RLN in relation to the inferior thyroid artery (ITA), the tracheoesophageal groove, Berry's ligament, and the inferior cornu of the thyroid cartilage is quite variable (567). Some of these anatomical features are a reliable landmarks in identifying the RLNs. Anatomical variations of RLN rarely can be identified preoperatively (789). Anatomical variations of RLN are associated with higher injury rates, because of difficult identification, challenging confirmation, and misidentification (123456789). This is definitely true for both open, endoscopic and robotic thyroidectomies.
In fact, early and definitive identification of RLN and its possible anatomical variations, or pathological RLN distortion by goiter, cancer, recurrence, or ITA is important to prevent injury. The bifurcated RLN represent a significant anatomical variation because prevention of VCP requires preservation of all branches of the RLN. An awareness of the surgical anatomy and the possible dispositions and ramifications of the RLN is very helpful in avoiding its injury during thyroidectomy.
The current report derives from a review of the literature and personal experience on identification, confirmation, and monitoring the bifurcated RLN.
PREVALENCE OF BIFURCATED RLN
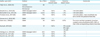
Reports on incidence of extralaryngeal branching present different rates, probably owing to the deep dissection into the inferior pharyngeal constrictor muscle, the inclusion of the ansa Galeni as a extralaryngeal branch, the association of branches to other organs (trachea, esophagus, etc.) and/or the use of accessories that simplify branches identification as loupe magnification, endoscope magnification, and intraoperative neural monitoring (IONM). Table 1 depicts prevalence of RLN ramifications reported in several studies.
Table 1
Prevalence of bifid RLN

| Author, year (ref.) | No. of RLN | Ramification (%) |
|---|---|---|
| Gregg, 1957 (10) | 669 | 61.3 |
| Katz, 1986 (11) | 721 | 58.3 |
| Katz and Nemiroff, 1993 (12) | 1,177 | 63.9 |
| Page et al., 2003 (13) | 251 | 23.0 |
| Wang et al., 2005 (14) | 63 | 76.0 |
| Beneragama and Serpell, 2006 (15) | 213 | 36.2 |
| Yalçin et al., 2006 (16) | 86 | 85.4 |
| Yalcin et al., 2008 (17) | 110 | 93.0 |
| Sancho et al., 2008 (18) | 302 | 37.0 |
| Casella et al., 2010 (19) | 195 | 18.5 |
| Cernea et al., 2009 (20) | 2,154 | 64.0 |
| Barczyński et al., 2016 (21) | 2,500 | 25.0 |
In a study, 721 RLN were visualized and 421 nerves (58%) bifurcated or trifurcated more than 0.5 cm from the cricoid cartilage. Ninety-seven patients had bilateral bifurcations, and 10 patients had trifurcations (11).
Beneragama and Serpell (15) examined the prevalence of extralaryngeal bifurcation of the RLN seen during thyroid/parathyroid surgeries. All patients undergoing total thyroidectomy, hemithyroidectomy and parathyroidectomy (excluding all minimally invasive procedures). Operative data obtained prospectively included the location of the nerve, number of branches, and the distance in millimetres from the inferior border of the cricothyroid to the point of bifurcation. A total of 213 (right=114, left=99) RLN in 137 patients were studied. Seventy-seven (36%) nerves bifurcated or trifurcated before entry into the larynx. Bifurcations were more common on the right (43%) than on the left (28%) (P=0.050). Trifurcations were seen in 8 nerves, seven on the right and one on the left (P=0.050). Bilaterally branched RLN were observed in 14 (18%) of 77 patients undergoing a bilateral procedure. One non-RLN was identified on the right. The median distance from the cricothyroid to the point of division was 18 mm on the right and 13 mm on the left (15).
Barczyński et al. (21) investigated the prevalence of the RLN branching: the bifid RLNs were identified in 613/2,500 (24.5%) nerves at risk, including 92 (7.4%) patients with bilateral bifurcations.
Sancho et al. (18) identified 2 extralaryngeal branches of the RLN in 97 nerves (32%) and 3 branches in 16 (5%), giving an overall prevalence of extralaryngeal branching of 37.4%. There were no significant differences in the prevalence of branching between the left and right sides, or between men and women (39% vs. 36%; P=0.595). The mean distance between the point of branching and the entrance of the RLN into the larynx was 21 (range 3–50) mm, with no significant difference between sides (18).
Casella et al. (19) in 2008 reported 36 of 195 (18.5%) nerves with extralaryngeal branching, 27 cases (25.5%) on the right and 9 on the left side (10.1%; P=0.009). Trifurcation of the RLN was identified in 2 dissections (1%) and bilateral bifurcations were observed in 3 of 80 (3.7%) patients (19).
Fontenot et al. (22) evaluated retrospectively the gender, race, and electrophysiologic features of branched RLN. Presence of RLN branching, its distance from the laryngeal nerve entry point (NEP), and functionality of the branches were ascertained. Patient demographics, rates of neural branching, and distance of bifurcation from the NEP were evaluated using statistical analysis. The author identified 719 RLNs at risk in 491 patients who underwent central neck surgery (22). Four-hundred and five (82.5%) patients were female and 86 (17.5%) patients were male. There were 218 (44.4%) African American patients and 251 (51.1%) Caucasian patients. In African American patients, 42.1% RLNs bifurcated compared to 33.2% RLNs in Caucasian (P=0.017) patients. The RLNs of African American and Caucasian patients bifurcated at comparable distances (P=0.300). In male patients, 39.1% RLNs bifurcated; whereas in female patients 36.2% RLNs bifurcated (P=0.530). On average, RLN bifurcation in female patients was at a longer distance from NEP compared to that of male patients (P=0.012). The authors concluded that African American patients have a higher rate of RLN bifurcation compared to Caucasian patients but no statistically significant difference in distance from NEP. Female patients tend to have longer branching variants of bifid RLNs (22).
Finally, Yalcin et al. (17) in 2008 proposed a classification for RLN ramification. In detail, 60 specimens (120 sides) were examined, including 41 men and 19 women cadavers between the ages of 40 and 89 years at death. In one right side, terminal segment of the nerve gave off many small branches surrounding the ITA then reaching the larynx, trachea, thyroid gland, and esophagus. In 8 sides, terminal segment of the nerve had no extralaryngeal division and entered the larynx as a single trunk. In 110 sides, the nerve had extralaryngeal division. One-hundred and three nerves had 2 laryngeal and 1 to 3 extralaryngeal branches. Two types were described in this group. In type I (66 nerves), both branches arose from the same level of nerve. Type I had 2 subtypes: 1) type Ia, the origin of the branches was just below the inferior constrictor muscle; and 2) type Ib, the origin of the branches was 15–35 mm below the muscle. In type II (37 nerves), the laryngeal branches arose just 3–5 mm above the extralaryngeal branches. We observed that the laryngeal and extralaryngeal branches arose generally from the same point of the RLN. The inferior laryngeal nerve is thus very short, or even nonexistent. Therefore, the authors even suggest that if the term “superior laryngeal nerve” is a given, standard, and accepted term, then the term “inferior laryngeal nerve” should also be accepted instead of the term “RLN” (17).
INJURY RATE OF BIFURCATED RLN
According to Barczyński et al.'s study (21), the prevalence of RLN injury was 5.2% vs. 1.6% for the bifid vs. non-bifid nerves (odds ratio [OR]=2.98; 95% confidence interval [CI]=1.79–4.95; P<0.001) in 1,250 patients who underwent total thyroidectomy with IONM.
Casella et al. (19) confirmed that the anatomical variation was more frequently associated both with unilateral permanent RLN palsy (relative risk [RR]=13.25; 95% CI=1.42–123.73; P=0.020) and unilateral transient RLN palsy (RR=7.36; 95% CI=1.84–29.40; P=0.006).
A prospective study assessed the impact of surgical injury and extralaryngeal branching of the RLN on vocal cord dysfunction (VCD), with 302 RLNs at risk (18). In all, 10.9% of patients developed VCD; had 4.3% paresis and 6.6% paralysis. All paretic and all but one paralytic cords recovered fully after 61 days. VCD was more frequently associated with branched than non-branched RLNs (15.8% vs. 8.1%; P=0.022). Injuries were more common in branched nerves (mean [standard error of the mean] of RLN, 0.94 (0.08) vs. 0.51 (0.05); P<0.001). Branched nerves were more likely to be associated with VCD (OR=2.2; 95% CI=1.1–4.5).
Therefore, branched RLNs suffer more surgical injuries and are twice as likely to be associated with VCD. There is no doubt that this anatomical variant must be identified early during thyroid dissection.
THE MOTOR FIBERS OF THE BRANCHED RLN
The function of the branched RLN was examined by microdissections, IONM and finger palpation (Table 2). Most studies reported that motor fibers are located exclusively in the anterior branch of the bifid RLN, but some objections and exceptions have been nicely reported. De facto, initially, studies reported that the motor component was present only in the anterior branch of the RLN, then with a better standardization of the IONM technique, motor proprieties were found in the posterior branch. Today, we can postulate that the functional anatomy of bifid RLNs demonstrated that anterior branches always contained motor fibres (100%) while posterior branches seldom contained motor fibres (0–8, 7%) (Table 2). The motor activity of the posterior branch is usually weaker than that of the anterior branch.
Table 2
Location of motor fibers within branches of the RLN
| Author, year (ref.) | Method | No. of RLN | Anterior branch motor | Posterior branch motor | Comments |
|---|---|---|---|---|---|
| Yalçin et al., 2006 (16) | Cadaver | 86 | + | + | - |
| Microdissection | |||||
| Microscope | |||||
| Serpell et al., 2009 (25) | IONM+laryngeal twitch | 176 | 100% | 0% | 1 mA stimulation |
| Barczyński et al., 2016 (21) | IONM+laryngeal twitch | 2,500 | 100% | 1.3% | 1 mA stimulation |
| Fontenot et al., 2014 (22) | IONM | 719 | 100% | 1.14% | 1 mA stimulation, mean amplitude was 634.5 mA for the posterior branches |
| Cernea et al., 2009 (20) | IONM | 2,154 | +++ | + | - |
| Cetin et al., 2016 (6) | IONM | 46 | 100% | 8.7% | The motor activity in posterior branches created a wave amplitude at 25%–69% of that in the corresponding anterior branches |
| Gurleyik, 2015 (23) | IONM | 61 | 100% | 12% overall | - |
| 18% right | |||||
| 8% left | |||||
| Uludag et al., 2016 (24) | IONM+laryngeal twitch | 200 | 100% | 8% | - |
| Kandil et al., 2011 (26) | IONM | 310 | 100% | 0% | - |
| Kandil et al., 2011 (27) | IONM | 137 | 100% | 0% | - |
Exhaustive microdissection descriptions were presented by Yalçin et al. (16) in 2006. In 49 specimens 96 sides were examined, including 27 male and 22 female cadavers. In 7 sides (7.3%, 5 on the left and 2 on the right) the RLN passed as a single trunk into the larynx below the inferior constrictor muscle. In 82 sides (85.4%, 40 on the left and 42 on the right) 2 laryngeal branches originated from the nerve. The nerve divided either just before entering the larynx (58.3%, 24 on the left and 32 on the right) or 15–32 mm below the inferior constrictor muscle (27.1%, 16 on the left and 10 on the right). In 69 sides (71.8%), the anterior and/or posterior laryngeal branches subdivided into 1 or 2 sub-branches. The anterior (observed in 49 sides, 51%) and posterior laryngeal branches supplied all intrinsic laryngeal muscles except the cricothyroid muscle and the mucosa below the vocal cords, respectively, while their sub-branches reached the cricopharyngeal part of the inferior constrictor muscle, esophagus and/or the thyroid gland. In 7 sides (7.3%, 4 on the left and 3 on the right) the nerve divided into 3 laryngeal branches (16).
Barczyński et al. (21) investigated the location of the motor fibers to the intrinsic muscles of the larynx among the bifid RLNs, and assess the prevalence of RLN injury with respect to nerve branching in a prospective cohort study of 1,250 patients who underwent total thyroidectomy with IONM. The primary outcome was the position of the motor fibers in the bifid nerves. Adduction of the vocal folds was detected by the endotracheal tube electromyography (EMG) and abduction by finger palpation of muscle contraction in the posterior cricoarytenoid. According to this investigation, the motor fibers of the RLN were located in the anterior extralaryngeal branch in the vast majority of but not in all patients. In rare cases, the motor fibers for adduction or abduction were located in the posterior branch of the RLN. In detail, the motor fibers were present exclusively in the anterior branch in 605/613 (98.7%) bifid nerves, and in both the RLN branches in 8/613 (1.3%) bifid nerves (21).
Fontenot et al. (22) evaluated 719 RLNs; electrophysiologic testing found motor fibers in all anterior branches and 3 posterior extralaryngeal RLN branches. Positive motor fiber stimulation correlated with an evoked glottis response waveform upon stimulation (22). In the 3 posterior branches with intraoperative nerve stimulation proven motor function, the mean amplitude of response to stimulation was 600 mA with mean latency of 1.2 msec. Each of these posterior branches produced a signal of comparable response characteristics to the one of the corresponding anterior branches (22).
Cernea et al. (20) nicely evaluated in 2010, 2,677 patients with intraoperative laryngeal nerve monitoring. A total of 1,390 RLNs (64.53%) had ramifications and the anterior branches usually exhibited more electrophysiologic activity.
Cetin et al. (6) evaluated 46 RLN with ramifications by IONM: motor activity was determined in all anterior branches. The functional anatomy of terminal branches detected motor activity in 4 (8.7%) posterior branches of 46 bifid RLNs. The motor activity in posterior branches created a wave amplitude at 25%–69% of that in the corresponding anterior branches.
Gurleyik (23) investigated the location of motor fibers within nerve branches by identifying motor function via IONM. Wave amplitudes were recorded after electrophysiologic stimulation. A total of 61 RLNs had bifurcation with anterior and posterior branches. Bifurcation occurred early along the pre-arterial (proximal) segment in 13% of bifid RLNs. IONM showed motor function in all anterior branches. IONM identified motor activity in 4 (18%) posterior branches of 22 right, 3 (8%) posterior branches of 39 left, and 7 (12%) posterior branches of all 61 RLNs with bifurcation. The rate of recorded wave amplitudes of motor function in 7 posterior branches was between 14% and 78% of those of corresponding anterior branches (23).
In another interesting study (24), anterior and posterior branches of the RLN were assessed separately by EMG (using a standard EMG endotracheal tube) for adduction and by finger palpation for abduction. The RLNs were classified as having motor function only in the anterior branches (group 1) or function both in the anterior and posterior branches (group 2). There were 185 RLNs in group 1 and 15 RLNs in group 2, assessed by intraoperative nerve monitoring. Motor function was detected in all anterior branches of the RLN (100%) and in 8% of the posterior branches. The mean branching distance was greater in group 2 compared with group 1 (24.1±13.6 mm and 17.3±8.5 mm, respectively; P=0.045). The authors concluded that although the anterior branch of RLN always has motor function, the posterior branch also has motor function in about 8% of patients. The probability of detecting motor function in the posterior branch was greater among early branching RLNs, which have a greater branching distance (24).
The data above are in contrast with Serpell et al. (25), Kandil et al. (2627) investigations. Serpell et al.'s study (25) aimed to establish the prevalence of extralaryngeal bifurcation of the RLN and investigate the location of the motor fibers to the intrinsic muscles of the larynx within the branches of the RLN in 579 patients undergoing thyroidectomy or open parathyroidectomy over a 3-year period. This was the first functional, in vivo study to demonstrate that the motor fibers for both adduction and abduction of the vocal cords are located in the anterior extralaryngeal branch of the RLN. Nerve integrity monitoring was utilized to document the position of the motor fibers of the last 176 RLNs. Adduction of the vocal cords was detected by the EMG endotracheal tube and abduction by finger palpation of muscle contraction in the posterior cricoarytenoid. A total of 838 RLN were studied (right 432, left 406). Bifurcations occurred on the right in 111 (25.7%) and left 93 (22.9%). Bilateral bifurcation occurred in 23 (8.9%) of bilaterally dissected nerves. Overall 176 RLNs in 118 patients were assessed by the nerve integrity monitoring. Of these 41 (23.3%) were bifid RLN. In all 41 (100%) cases of bifid RLN, motor fibers for both adduction and abduction of the vocal cords were located exclusively in the anterior branches of RLN, and none in the posterior branches.
In a first study by Kandil et al. (26), a total of 137 (right 69, left 68) RLNs in 99 patients undergoing thyroidectomy (total 29, hemi 51), parathyroidectomy (16), and central lymph node dissection (3) were studied (26). Overall, 46 RLNs (34%) bifurcated prior to entry into the larynx. These bifurcations occurred on the right in 27 (59%) and left in 19 (41%). Bilateral bifurcation occurred in 12 (27%) of the 44 patients who underwent bilateral dissections. The median branching distance from the cricothyroid membrane on the right was 8.3±2.5 mm, and on the left was 7.5±1.8 mm. In all bifurcated RLNs, the motor fibers to the vocal cords were located exclusively in the anterior branches. In a subsequent study by same group (27), 310 RLNs were collected. There were 133 RLNs (42.9%) that bifurcated before entering the larynx. These bifurcations occurred 51.1% on the right, 48.9% on the left, and 33.3% bilaterally. The median branching distance from the cricothyroid membrane on the right was 6.33 mm, and on the left was 6.37 mm. In all bifurcated RLNs, the motor fibers were located exclusively in the anterior branches (2627).
NEURAL MONITORING
Definitely, an algorithm and/or a standardized method and approach for monitoring the bifid RNL is missing. Table 3 summaries our suggested steps for identify and monitoring the bifurcated RLN.
Table 3
Suggested steps for identify and monitoring the bifurcated RLN

| 1. | Neural monitoring by endotracheal tube to detect adduction of the vocal cords in combination with finger palpation in the postcricoid space to detect posterior cricoarytenoid abductor function is useful the detect RLN ramification proprieties. |
| 2. | Use monopolar ball tip stimulation probe. |
| 3. | The bifurcation can occur at the level of the ITA. RLN should be localized and identified definitely with IONM proximally to the level of the ITA, to identify proximal ramifications to ITA. |
| 4. | Map and identify the RLN with IONM probe by stimulation intensity of 2–3 mA. |
| 5. | Once identified, trigger the nerve for functional and definitive confirmation with stimulation intensity of 0.5–1 mA. |
| 6. | The reduction of the nerve stimulation from 2–3 mA to 0.5–1 mA is essential to discriminate the motor component of the inferior laryngeal nerve, and mistaking a posterior branch of the RLN as the whole RLN, which inevitably places at risk an unidentified anterior branch containing all the motor fibers. Some sensitive ramifications in fact will respond as if motor, when overstimulation at 2–3 mA. |
| 7. | If it is not perceived any EMG response or laryngeal twitch, this is the sensory branching of the RLN. Therefore, the surgeon must explore for the motor branch, usually in a more ventral position. |
| 8. | When identified the branches, stimulate both ramifications with 0.5–1 mA with simultaneous laryngeal twitch to appreciate the motor component of each division. |
| 9. | If ramifications are very close together, almost parallel, it is advisable to stimulate with 0.5 mA to avoid shunting between the branches. De facto, in case 2 structures run close together (anterior and posterior branches of the RLN, or a small artery and RLN), a false EMG signal can be induced by a shunt stimulus, we lower the stimulation level to 0.5 mA under bloodless conditions (32). In this context, it seems to be reasonable and adequate to lower the stimulation to 0.5 mA if one wants to differentiate a motor branch from a sensory branch, or a small artery from the RLN. |
| 10. | When motor, posterior branch may present wave amplitude and latency but weaker than that in the anterior branch and laryngeal twitch. |
| 11. | In some circumstances, the anterior branch of the RLN can be stretched forward by Berry's ligament. It often swerves anteriorly within Berry's ligament and can appear like a small artery (32). |
| 12. | The diameter of the posterior branch of the RLN can sometimes be larger than that of the anterior branch. |
| 13. | Use the stimulating probe as a dissecting tool. |
| 14. | Preserve all RLN branching. |
The first randomized clinical trial of visualization vs. neuromonitoring of RLNs during thyroidectomy was published by Barczyński et al. (28) in 2008. Nerve monitoring decreased the incidence of transient but not permanent RLN paresis compared with visualization alone, particularly in high-risk patients. The prevalence of transient RLN paresis was lower in patients who had RLN monitoring by 2.9% in high-risk patients (P=0.010) and 0.9% in low-risk patients (P=0.250). Moreover, nerve monitoring helped to identify 33% more RLN bifurcations than visualization alone (33.8% vs. 24.6%; P=0.010). In Barczyński et al.'s study (28), nerve monitoring was able to help by confirming the location of the RLN motor component. As a bifurcated RLN is particularly prone to injury near the ITA or ligament of Berry, where it usually starts to bifid, the posterior sensory branch may be mistaken for the entire RLN, causing the injury of the anterior motor branch.
In a subsequent opinion letter, Barczynski and his colleagues (29) noted that in 230 nerves at risk, 63 bifid RLNs, and in all except one patient, the author found both a positive nerve monitoring response and laryngeal twitch response when stimulating the anterior branch of RLN. However, in 1 case, stimulation of the anterior branch of RLN resulted in a positive nerve monitoring response, but a negative laryngeal twitch response, which was positive during stimulation of the RLN posterior branch (29). It is important to stress that laryngeal palpation complements electromyographic monitoring, which should be used together at least in all cases of bifid RLNs.
Again, Barczynski et al. (30) evacuate the clinical utility of IONM to detect RLN ramification. Among patients operated with vs. without IONM, the early RLN injury rate was 3% vs. 6.7% (P=0.020), including 2% vs. 5% (P=0.040) of temporary nerve lesions, and 1% vs. 1.7% of permanent nerve events (P=0.310), respectively. Extralaryngeal RLN bifurcation was identified in 42 (27.8%) vs. 25 (16.6%) of patients operated with vs. without IONM, respectively (P=0.001).
A branched RLN is at greater risk of injury and highlighted the dangerous potential situation of mistaking a posterior branch of the RLN as the whole RLN, which inevitably places at risk an unidentified anterior branch containing all the motor fibers.
Neural monitoring by endotracheal tube to detect adduction of the vocal cords in combination with finger palpation (31) in the postcricoid space to detect posterior cricoarytenoid abductor function is useful the detect RLN ramification proprieties. IONM aid preservation of an anterior RLN branch. IONM significantly aids visual identification of RLN, allowing even for nerve mapping before its visualization, and provides the surgeon with a functional dimension previously not available with visual identification alone. It is clear that the use of IONM has led to the important findings of adductor and abductor motor function within the anterior branch and the significance of anterior branch identification in bifid RLNs. IONM may help to differentiate between motor and sensory functions of nerve branches. The morphology and functional anatomy of all nerve branches must be preserved to ensure a safer surgery.
The branching pattern of the nerve may be important pitfalls of the thyroidal and laryngeal surgery. Owing to this the surgeon should keep in mind the risk of extra laryngeal division of the nerve and not confuse laryngeal and extra laryngeal branches.
The length of the branch also appeared to be related to the risk of VCP. The thinner anterior branch had to cope with a similar or greater amount of manipulation/mobilization stress than its single-trunk counterpart and being more vulnerable, is associated with a higher proportion of dysfunctional cords. The greater vulnerability of a branched RLN and the importance of preserving every branch of the RLN has been recognized previously. The belief of some surgeons that injury to one branch of a nerve can be compensated by the other branch is by no means supported by the clinical findings. Greater awareness of the increased vulnerability of branched nerves, together with the increased availability of intraoperative monitoring of the RLN, should help further to reduce the rate postoperative VCP.
IONM provide anatomical functional dynamics that allows for the location and confirmation of the RLN motor and sensory fibers. Standardized reports provided evidence that the RLN motor fibers occur in all anterior RLN branches and rarely in the posterior branch of the RLN. IONM may be useful to discriminate the motor component and characteristics (adduction or/and abduction) of the bifid RLN. IONM allow early differentiation and confirmation of a branched nerve. Anatomical variation identification and quality of RLN dissection is improved with IONM technology. Unseen branches of the RLN are at risk of injury during surgery. Therefore, great care is required following presumed identification of the RLN to ensure that there are no other unidentified branches. IONM enhances the gold standards for intraoperative RLN management, that is extensive knowledge of RLN anatomy, identification of RLN, and exposure of RLN. Great caution is required after the presumed identification of the RLN to ensure the presence of branches with functional (IONM) verification.
CONCLUSION
Most studies show consistently that bifurcated RLN occur frequently (11121314151617181920). The bifurcated RLN is associated with a clearly higher VCP risk (32). As the bifid nerves are more prone to injury than non-branched nerves, meticulous dissection is recommended to assure preservation of all the branches of the RLN during thyroidectomy (12). The anterior branch of the RLN constitutes the motor pathway. The posterior branch of the RLN is rarely motor-relevant. RLN motor fibers reside primarily in the anterior branch but may occur in the posterior branch (14). Wave amplitude analysis showed that motor function in the posterior branch is weaker than that in the anterior branch (32). Careful microdissection in the particularly vulnerable section of the nerve pathway between the point of intersection and the nerve entrance is therefore of particular importance in total thyroid resection in order to avoid postoperative VCP (32). On the basis of the location of motor fibers in both branches, total exposure and preservation of anatomy and function of all branches of the RLN is mandatory for complication-free thyroid surgery (15).
Electrophysiologic testing may be as an important adjunct to visualization of the nerve with this anatomic variation. Further studies with a large number of patients are needed to clarify the electrophysiological correlates of the evoked electromyographic, as well as laryngeal twitch response in relation to the anatomic variability of RLNs (32). This issue is of great clinical importance and we should realize that branched nerves are particularly prone to injury, which should oblige the surgeon to exercise the greatest effort in identifying and preserving every branch of RLN (20).
The aid of IONM nowadays plays an ever increasing role in the surgical armamentarium and it should be helpful to further reduce the prevalence of RLN dysfunction (Table 3). IONM can 1) early identify a branched RLN, 2) distinguish the 2 components both motor and sensitive proprieties of branches, and 3) aid in branches dissection (Table 3). The use of IONM may improve the outcomes of surgery among these patients by both increasing the completeness of total thyroidectomy and significantly reducing the prevalence of temporary RLN injury (32). The possible mechanism of this improvement is the aid in dissection at the level of the Berry's ligament offered by IONM which enhances the surgeon's ability to identify a branched RLN, and allows for reduction of traction injury and neuropraxia of the anterior and posterior branches of bifid nerves (Table 3).
 XML Download
XML Download