

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Papillary thyroid cancer (PTC) is the most common endocrine neoplasm arising from thyroid follicular cells and its incidence is tending to increase (1). Although the prognosis for most patients with PTC is excellent, up to 35% of patients suffers from the disease recurrence during a 40-year follow-up period (2). Upon considering recent expectancy treatment strategy (wait and see) recommended for clinically low-risk patients with PTC, identifying high-risk PTC patients in the early stage of the disease is important in order to reduce the chance of tumor recurrence (3).
Recently, B-type Raf kinase (BRAF)V600E mutation has emerged as a promising prognostic factor for the patients with PTC (4). The BRAF mutation is common in PTC, with a frequency of approximately 45% (ranging, 27%–87%) (56). The BRAF mutation has been reported to be associated with poor prognosis owing to its aggressive clinical features, such as extra thyroidal invasion, lymph node (LN) metastasis, advanced tumor, node, and metastasis (TNM) stage, and nodal recurrence (578). However, the clinical significance of BRAF mutation for predicting poor PTC prognosis has been controversial in a way that a number of authors have reported this mutation was not associated with aggressive behavior or poor prognosis (91011).Therefore, in this study, we evaluated the association between the BRAF mutation and pathologic aggressiveness (or the clinical significance) in the BRAF mutation patients with PTC.
METHODS
1. Patients' selection
We consecutively enrolled 1,503 patients with PTC who had undergone surgery as the initial treatment for thyroid cancer and BRAF mutation test altogether who had registered between January 2009 and October 2013.
2. Surgical strategy
The thyroid surgeries were performed according to the 2006 American Thyroid Association (ATA) guidelines for differentiated thyroid cancer management. Thyroid lobectomy and isthmectomy were performed if the cancer was an unifocal intrathyroid microcarcinoma (≤1 cm) with no cervical LN metastasis. In other cases, total thyroidectomy was performed. Central compartment node dissection was also performed routinely in patients with PTC. Prophylactic central compartment dissection was performed in these patients, even though central LN metastases were not suspected clinically. When lateral LN metastasis was identified during preoperative or intraoperative evaluation, comprehensive neck dissection (level II–V) was performed.
3. Scintigraphy protocol
Radioactive iodine (RAI) remnant ablation was performed with the same indications as for those with total thyroidectomy. Patients did not take levothyroxine for 4 weeks, but took a T3 supplement for first 2 weeks instead. Then they were instructed to follow a low-iodine diet for the remaining 2 weeks. The therapeutic dosage of 131I was 1.1–5.5 GBq for 3–6 months after total thyroidectomy.
4. Thyroglobulin (Tg) and Tg antibody measurement
The 1st pre-RAI stimulated thyroglobulin (sTg) was checked at 1 week before the 1st RAI. Because it reflects the effect of surgery, it is named as a postoperative sTg. The 2nd RAI sTg was measured at between 6 months to 1 year after the 1st RAI. This reflects the treatment outcome of 1st RAI therapy, therefore it is named as a post-RAI therapy. The clinical efficacy of RAI therapy has been demonstrated in cancers with tumors greater than 4 cm or with distant metastases, but no clinical effect has been demonstrated in the intermediate-risk group. However, we did not completely rule out the effects of RAI therapy on cancer and classified it into 2 groups in order to avoid the bias being caused by the RAI therapy. The IRMAZENco Tg-S Kit® (ZenTech, Liege, Belgium) was used to check sTg. The functional sensitivity of the kit was lower than 0.1 ng/mL with 20% maximum inter-assay variation. Serum anti-Tg antibody was measured by immunoradiometric assay® (anti-Tg RIA; BRAHMS, Henningsdorf, Germany) and the functional sensitivity was ≤20 IU/mL with a 20% inter-assay variation coefficient. In this study, anti-Tg antibody levels ≤100 IU/mL were regarded as negative and anti-body levels >100 IU/mL were excluded from our data analysis.
5. Recurrence
Recurrence was defined as a biopsy-proven tumor after having free of disease for 6 months clinically after the initial therapy, or detection of a new lesion on follow-up imaging studies with Tg level ≥2 ng/mL. Biochemically persistent disease with Tg level ≥2 ng/mL without evidence of radiologically proven disease after the initial treatment was not considered recurrence.
6. DNA extraction and molecular analysis of BRAF mutation
Formalin-fixed, paraffin-embedded tissue blocks were sectioned at 10-μm thickness, and DNA extraction were performed with QIAamp DNA FFPE Tissue Kit® (Qiagen, Hilden, Germany) following the manufacturer's instruction. The BRAFV600E mutation was analyzed according to the procedure of Hayashida et al. (12). Specific primers for exon 15 of the BRAF gene (5′-ATAGGTGATTTTGGTCTAGCTCCGG-3′ and 5′-GATTTTTGTGAATACTGGGAACT-3′) were used to amplify a 210-bp gene fragment. The reaction began with denaturation for 5 minutes at 95ºC, followed by 30 cycles of replication and final extension at 72ºC for 5 minutes using a TaKaRa PCR Thermal Cycler Dice® Gradient (TaKaRa Bio Inc., Mountain View, CA, USA). The polymerase chain reaction (PCR) products were digested by the restriction endonuclease BspEI® (10 U/μL; New England Biolabs, Beverly, MA, USA) for 15 minutes, which was used to identify the BRAFT1799A mutation as follows. The BspEI® enzyme digested the PCR product to produce one major band (189 bp) from the wild-type allele (210 bp). The PCR products were electrophoresed in Agarose SFR® (Amresco, Solon, OH, USA) after Ethidium bromide staining and the gels were photographed under UV trans-illumination using Gel Doc XR® (BIO-RAD, Hercules, CA, USA).
7. Statistical analysis
We compared the patients' clinicopathological features using Student's t-test, χ2 tests, and Fisher's exact test except postoperative and post-RAI sTg for the Wilcoxon rank sum test. We analyzed recurrence-free rate, which was assessed from the date of initial surgery to time of recurrence using the Kaplan-Meier method and the Cox regression test. All tests were 2-sided, with an alpha level of 0.05. We performed all calculations using SPSS 17.0® (SPSS Inc., Chicago, IL, USA). This study was approved by our institutional Research Ethics Committee.
RESULTS
The patients with the BRAF mutation had more frequent classic subtype of PTC, extrathyroidal invasion, T3 stage, N1a stage and TNM stage III compared to those without the mutation. In postoperative & post-RAI serum Tg levels, the number of patients was somewhat different from the number of RAI treatment. Because other types of cancer might have occurred or the patient had wanted to stop the treatment because of difficulty of enduring the treatment or old age. The frequency of both total thyroidectomy and RAI was not different between the 2 groups (Table 1). And, as shown in Fig. 1, the recurrence-free rate was not different between the 2 groups. Although the BRAF mutation had aggressive features, it did not affect the prognosis among these patients. Therefore, we searched for prognostic factors and performed subgroup analysis to evaluate why the recurrence was not different between the 2 groups. The N stage, number of central metastatic LNs, number of total metastatic LNs, postoperative sTg and post-RAI sTg were found out to be the significant prognostic factors in univariate analysis, but post-RAI sTg was the only prognostic factor in multivariate analysis in these patients. However, among the patients who did not undergo RAI therapy, both the N stage and the number of central metastatic LNs were the significant prognostic factors in univariate analysis (Table 2). The cut-off levels of postoperative sTg and post-RAI sTg in our institution were shown at Table 3. The differences of cut-off level may be attributable to the different characteristics of the enrolled patients, which we will investigate in the future. Then, we performed subgroup analysis with the post-RAI sTg, N stage, and number of central metastatic LNs. In patients who had undergone RAI, their post-RAI sTgs were not different between those with and without mutation. In patients who did not undergo RAI, the N1a stage was more frequent in patients with the mutation than those without, but the frequency of ≥5 metastatic LNs did not differ between the 2 groups of with and without the BRAF mutation (Table 4). The 9 patients with N1b stage who did not undergo RAI had skip metastasis without LN metastasis at central compartment and had fewer 5 metastatic LNs.
Table 1
Clinicopathological features of patients with and without the BRAF mutation

Data are shown as mean±SD, number (%), or median value (number of patients).
BRAF = B-type Raf kinase; PTC = papillary thyroid cancer; TNM = tumor, node, and metastasis; LN = lymph node; RAI = radioactive iodine; sTg = stimulated thyroglobulin; SD = standard deviation.
*sTg cases with thyroglobulin antibody <100 ng/mL are analyzed.
Fig. 1
Recurrence-free rate was not different between the groups with and without the BRAF mutation.
BRAF = B-type Raf kinase.
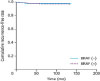
Table 2
Univariate and multivariate analyses of prognostic factors

Table 3
Receiver operating characteristic curve analysis of postoperative, post-RAI sTg, and number of metastatic LNs

| Variables | AUC (±SE) | Optimal cut-off point | P value | |
|---|---|---|---|---|
| ① vs. ③ | ② vs. ③ | |||
| Postoperative sTg (①) | 0.882 (±0.030) | 2.7 | 0.997 | 0.998 |
| Post-RAI sTg (②) | 0.846 (±0.028) | 5.6 | ||
| No. of metastatic LNs (③) | 0.794 (±0.025) | 5.0 | ||

DISCUSSION
BRAF mutation is the most common genetic alteration in PTC. The causal role of this mutation in tumor initiation has been confirmed in transgenic mice with BRAF mutation however its poor prognostic effect is controversial (13). In our study, the patients with BRAF mutations had more aggressive pathological features such as extra thyroidal invasion, T stage, N stage, TNM stage and the number of metastatic LNs than those without the mutation, which was also found same in other studies (5678).
The patients with the mutation had higher T, N, and TNM stage than those without the mutation in our study. Although these aggressive pathologic features were associated with recurrence which was not different between the patients with and without BRAF mutation in this study. Likely, shown in our study, some other studies have also demonstrated that the mutation is not an independent prognostic factor for the recurrence in multivariate analysis (141516). As far as we know, no study on the prognostic value of BRAF mutation in PTC patients was ever performed incorporating the response of treatment, which can explain the discordance between the aggressiveness and the prognostic effect of BRAF mutation. Post-RAI sTg is known as a prognostic factor for the recurrence and a response value to treatment in patients with well-differentiated thyroid cancer (17). In our study, post-RAI sTg was the only prognostic factor for the recurrence and showed similarity between the 2 groups. In the RAI undergone group with or without BRAF mutation, it was seen that the sTg (which reflects the treatment result) was similar. In other words, although the patients with BRAF mutation had more aggressive pathologic features than those without, the risk of recurrence of the group with BRAF mutation was reduced to the same as the group without after thyroid surgery and RAI therapy. In the group that did not receive RAI therapy, the N stage and number of central metastatic LNs were important prognostic factors, which reflected aggressive behaviors of the tumor. In this group, the recurrence rate was similar between the 2 groups because most patients (99.6%) in this group were in early stages of the disease having less than 5 metastatic LNs. In addition, the frequencies of N1b and number of ≥5 metastatic LNs between the 2 groups were similar as shown in Table 3. In other words, the similar recurrence rate, shown in between the 2 groups who had not undergone RAI therapy, was attributed to the fact that the patients with BRAF mutation might have been treated in early stages. In summary, although tumors in the group with the BRAF mutation showed more aggressive behavior, the patients with and without the mutation can have similar outcomes if both are treated early when the N stage has not yet reached N1b nor ≥5 metastatic LNs, and the level of post-RAI sTg can be guaranteed in patients without the BRAF mutation.
Recently, the active surveillance approach is a safe alternative to the early treatment advocated by Ito et al. (18) and Sugitani et al. (19). Surgical interventions were necessary in about 15% patients among them for the period of 10 years follow-up. In the new era of 2015 ATA guidelines, which adopted the wait and see strategy in low-risk PTC, there still pertain a dilemma of how aggressively low-risk patients need to be treated. Although BRAF mutation is not a prognostic factor for recurrence after initial appropriate treatment, BRAF mutation may be used for a preoperative modulator for the determination of early surgical intervention because of its relationship between BRAF mutation and aggressive tumor behavior as shown in a number of previous studies (202122).
In our institution, surgery had been preferred to the active surveillance in patients with less than 1 cm of thyroid cancer until 2012. Therefore, the recurrence rate of patients with BRAF mutation was not higher than those without the mutation even though the BRAF mutation had aggressive behavior in this study. Thus, this mutation may help surgeons to determine the extent of thyroid surgery especially in the prophylactic central LN dissection (23). However, other oncogenic mutations will be evaluated in order to identify more specific markers of less favorable PTC outcome in the future, because the BRAF mutation had a low positive predictive value and about 50% patients with BRAF mutation had no LN metastasis (202122). The limitations of this study are the short follow-up time and the sensitivity and specificity were not as good as direct DNA sequencing analysis even though the PCR-restriction fragment length polymorphism (RFLP) was a useful method for BRAF mutation. Another additional limitation of this study is that the suppressed Tg level is not included in more significant prognostic value for the recurrence.
In conclusion, the BRAF mutation was correlated with aggressive behavior but it was not a prognostic factor for recurrence in this study possibly because of early surgical intervention and similar response to the treatment. Therefore, it is important to determine possibilities of early surgical intervention among the patients with the BRAF mutation and it may be a useful preoperative modulator to determine whether early surgical treatment is necessary or not in which shows more aggressive behavior and LN metastasis.
 XML Download
XML Download