

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The regular questioning of the benefit of general prophylactic antibiosis is an important issue. Because of the anxiety with respect to postoperative complications, especially in elective surgery, many surgeons tend to prescribe antibiotics thereby neglecting the adverse side effects of this medication (1). Furthermore, such treatment might support the development of antibiotic-resistant colonies and might involve unnecessary expenditure for the individual or for the health care system (2). Thus, the general question needs to be raised as to whether antibiotic prophylaxis is necessary in thyroid surgery.
Surgical site infections (SSIs) are potential complications related with all surgical procedures, and perioperative antibiotic prophylaxis are used to prevent SSI (3). The prevalence of chronic pulmonary and liver disease, prior radiation therapy, immunological dysfunction, and anemia in the thyroid disease population may contribute to delayed wound healing and SSI (4). However, thyroid surgery is classified as a clean surgical procedure according to the international surgical wound classification and is associated with a low incidence of SSI, therefore, international guidelines do not recommend routine perioperative antibiotic prophylaxis (5). Despite this evidence, many of endocrine surgeons continue to use perioperative antibiotics (6). We undertook this investigation to ascertain the role of perioperative prophylactic antibiotics during thyroid surgery. The purpose of this study is to evaluate the therapeutic benefits of using perioperative antibiotic prophylaxis in thyroid surgery by comparing groups with and without perioperative antibiotic prophylaxis.
METHODS
This retrospective study evaluated medical records of 1,895 patients who underwent thyroid surgery at the Gangnam Severance Hospital between January 2013 and December 2013. Both patient factors such as sex, age, body mass index (BMI), and comorbidity and surgical factors such as operation time, drain removal day, postoperative complications, operation type, incision length, operation device, and node dissections were included in analysis. To minimize variations among operators, cases only in a single institute and by a single surgeon were included. Prophylactic antibiotics were used before June 2013 and no prophylactic antibiotics were used from July 2013 to December 2013. Closed drainage tubes drained by negative pressure were inserted into all the patients after the surgery and the tubes were removed when the amount of daily drainage is less than 30 mL. Surgeries using endoscope or robot-assisted surgeries were excluded in this study. Operation device were categorized as conventional method, electro-thermal dissecting tool (Ligasure™ curved small Jaw; Covidien, Mansfield, MA, USA), and ultrasonic dissecting tool (Harmonic Focus®; Ethicon Endo-Surgery, LLC, Cincinnati, OH, USA) for the analysis. Skin incision lengths were categorized as less than 5 cm and longer than or equal to 5 cm. Operation type was classified as total thyroidectomy (TT) and less than TT. Node dissection was classified as central compartment node dissection (CCND) group and lateral neck node dissection (LND) group. For surgical suture, a braided synthetic absorbable suture, Vicryl™ 4-0 (Ethicon Endo-Surgery, LLC), was used and a monofilament synthetic absorbable suture, Maxon™ 5-0 (Covidien), was used for dermal suture. Nonabsorbable Sofsilk™ 3-0 (Covidien) sutures was used for tagging drainage tube in the skin. Statistical analysis was performed by National Health Insurance Service Ilsan Hospital Medical Research Center and statistical significance was defined as the P value less than 0.05.
The study protocol was approved by the Institutional Review Board of the Gangnam Severance Hospital (Yonsei University College of Medicine, Seoul, Korea). Owing to the retrospective nature of the study, neither patient approval nor informed consent was required.
RESULTS
The male to female ratio was 1:3.3, the average age was 43 (14–82) years old, and the average BMI was 23.4 kg/m2 (16.02–63.23). The numbers of subjects without and with antibiotic prophylaxis were 593 and 1,303, respectively, resulting in ratio of 1:2.2. In Table 1, patient factors were analyzed comparing between groups with and without antibiotic prophylaxis. Similarly, surgical factors were analyzed as shown in Table 2. Age and BMI showed no difference between the groups, whereas operation time in antibiotic prophylaxis group was longer than the group without antibiotic prophylaxis. We consider such difference comes from the fact that antibiotic prophylaxis was used in patients who are expected to require longer procedure time based on the preoperative radiological examinations. Drain removal day was longer in the group without antibiotic prophylaxis even though the difference was not statistically significant. Six cases (1%) of postoperative complications were reported in the group without antibiotic prophylaxis including 3 cases of chyle leakage, 2 cases of SSI, and 1 case of nerve injury. In the group with antibiotic prophylaxis, 31 cases (2.4%) were reported including 15 cases of chyle leakage, 8 cases of SSI, and 8 cases of nerve injury. Postoperative bleeding was not reported in both groups. Since patients expected with high risk of postoperative complications were treated with antibiotic prophylaxis, we consider that resulted in those statistical significance. Operation type also showed statistical significance between the groups because more TTs were undergone in the group without antibiotic prophylaxis compared to the group with antibiotic prophylaxis (83% vs. 63%). Incision length and node dissection showed statistical significance as well due to the fact that antibiotic prophylaxis was used in patients with longer incision length or extended node dissection. Operation device also has statistical significance because more conventional method was used in the group without antibiotic prophylaxis (90%), whereas ultrasonic dissecting tool was more used in the group with antibiotic prophylaxis (30%) compared to the group without antibiotic prophylaxis. In Table 3, patient factors with SSI were analyzed comparing groups with and without antibiotic prophylaxis and there was no statistical significance between 2 groups. In Table 4, surgical factors with clinical outcomes related with SSI were analyzed comparing groups with and without antibiotic prophylaxis. Similar to the patient factors comparison in Table 3, no statistical significance was observed.
Table 1
Comparison between without and with antibiotic prophylaxis group according to patient factors

Table 2
Comparison between without and with antibiotic prophylaxis group according to surgical factors

Table 3
Comparison between patient factors and antibiotic prophylaxis among patients who showed SSI
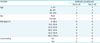
Table 4
Comparison between surgical factors and antibiotic prophylaxis among patients who showed SSI

DISCUSSION
A SSI is defined as infection related with the surgical procedure and occurs within 30 days after the operation (4). According to the guideline by the Centers for Disease Control and Prevention (CDC) in 1999, more than 30 million of surgical procedures are performed each year in the United States with reports that 2%–3% of the cases have SSI, although actual incident rate of SSI is suspected to be much higher (5). SSIs account for one fourth of all nosocomial infections (7).
Thyroid operation is classified as a clean procedure and the incidence of SSI is relatively low (0.3%–2.9%) resulting in that routine perioperative antibiotic prophylaxis is not recommended except for certain conditions (8910). However, higher number of perioperative antibiotic prophylaxis is reported in the United Kingdom (25%), Italy (50%), and China (57.4%–100.0%), probably due to precautions against the chance of SSI (10111213). In this study, 2 cases (0.08%) and 8 cases (0.6%) of SSIs were reported in the groups without and with antibiotic prophylaxis, respectively.
Patient factors and operative factors are associated with an increased risk of an SSI (6). Patients with SSI were divided into 2 groups, with and without perioperative antibiotic prophylaxis, and analyzed by patient factors such as age, sex, BMI, and comorbidity, and by operative factors such as operation time, drain removal day, postoperative complications, operation type, incision length, operation device, and node dissection (Tables 3 and 4). Age had no correlation in both groups, and in contrast to the report that age is one of the risk factor for SSI, no SSI was reported in patients over 65 years old (1). Moreover, in contrast to previous studies that show patients with high blood pressure or diabetes that suppress immunity have higher incidence of SSI, no SSI was reported in both groups in this study (1415).
Obesity is one of the risk factors for SSI and World Health Organization (WHO) categorizes obesity according to the BMI (16). In this study, 2 SSI cases were reported in normal BMI (18.5–24.9 kg/m2) in the group without perioperative antibiotic prophylaxis, whereas 5 and 3 SSI cases were reported in normal BMI (18.5–24.9 kg/m2) and pre-obese BMI (25.0–29.9 kg/m2), respectively, in the group with perioperative antibiotic prophylaxis without statistical significance. All patients with SSI had no other postoperative complications. Although hematomas by postoperative bleeding are known to increase the risk of SSI, no postoperative bleeding was reported in this study (17).
Perioperative prophylactic antimicrobial agents are administered as a single dose 30–60 minutes prior to operation and additional dose may be administered provided the operation time exceeds 4 hours (18). Despite the studies reporting association between operation time and SSI, no statistical significance was observed in this study (19). Although the average operation time of the groups with and without perioperative antibiotic prophylaxis are 107 and 99 minutes, respectively with statistical significance, no patients required more than 4 hours of operation time and consequently additional antibiotics were not needed. In this study, incision length and SSI has no correlation because the incision length was smaller compared to other surgeries. Association between suture material and SSI has been reported in many studies and instead of conventional method using suture material, various operation devices have been introduced to reduce operation time and infection due to foreign-body reaction of suture material (2). No correlation between operation device and SSI was observed in this study. Node dissection has been known to be a risk factor of SSI in thyroid operation (1720). In this study, however, CCND was performed in all cases and additional LND was performed in 53 cases (9%) and 159 cases (12.2%) in groups without and with perioperative antibiotic prophylaxis, respectively, showing no statistical significance associated between SSI and node dissection in groups with and without perioperative antibiotic prophylaxis. Drainage tubes are implanted after surgery to remove hematoma or serous fluids in surgical sites. Although drainage tubes may serve as a risk factor of SSI, closed drainage tube placed away from the skin incision site has decreased chance of SSI compared to otherwise (3). In thyroid operation, drainage tube and SSI was reported to have little correlation (21). In many cases of thyroid operations, drainage tubes are implanted to detect complications such as bleeding, and in this study, closed drainage tubes were used as for the same purpose in all subjects followed by removal of the tube when the amount of drainage is less than 30 mL (22). In both groups, SSI was reported when the drainage tube was remained more than 3 days even though the difference was not statistically significant. As aforementioned, validity of perioperative antibiotic prophylaxis was evaluated by analyzing patient factors and surgical factors. Results of this study indicate that clinical outcomes have no significant differences between groups with and without perioperative antibiotic prophylaxis in thyroid surgery. In thyroid surgery, perioperative antibiotic prophylaxis may not be required routinely once the surgical procedure underwent with aseptic condition and the patients care was performed appropriately. Nevertheless, several factors such as smoking, steroid administration, or malnutrition that increase incidence of SSI by delaying surgical wound healing or suppressing immunity were not included in this study (232425). Moreover, all subjects were implanted with closed drainage tubes resulting in absent of analysis for patients without drainage tubes. Future studies with additional factors may provide more reliable results.
 XML Download
XML Download