

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The nature and indication for drain insertion after thyroid surgery vary and the perceived risk of hemorrhage and drainage of lymphatic fluid is the major reason why drains are frequently inserted. Drainage tubes are usually inserted in individuals with severe thyroiditis, with a bleeding tendency, or in those who have gone through a lymph node dissection. An open drainage tube was often inserted into the neck cavity after thyroidectomy to drain collected excess fluid. Retained drains are an infrequent and usually avoidable postsurgical complication. Inadvertently, a drainage tube fragment was left at the time of removal in a patient and it was detected as a palpable neck mass on a follow-up examination 18 months after the operation. In the current report, we present this case.
CASE REPORT
A 61-year-old female patient presented with a one-year history of a mass on the anterior neck 2 years ago at a local hospital. A physical examination displayed a soft, movable mass measuring 2.0 cm. A neck ultrasonography (US) revealed multiple masses on both thyroid glands. The largest one was a 2.0×1.4 cm sized well-defined isoechoic mass in the right lobe of the thyroid gland and the second-largest a 0.8×0.9 cm sized mass in the left thyroid gland with an irregular border. Fine needle aspiration cytology was performed in the left thyroid nodule and the results revealed a papillary thyroid carcinoma.
The patient underwent a total thyroidectomy with a central lymph node dissection at a local hospital. A Penrose drain was placed into the surgical bed through the wound and removed 24 hours after the operation. There were no problems and she was discharged 2 days after the surgery.
The patient was followed up in an out-patient clinic and thyroid hormone was supplemented with Levothyroxine. She revealed a new lesion on the anterior neck 18 months after the operation and was transferred to our hospital for further treatment. The clinical examination revealed a 1.5 cm sized firm nodular mass on the anterior neck. Neck US was conducted and a lateral soft tissue neck radiograph examined. Neck US revealed a hypoechoic lesion with tubular-shaped parallel hyperechoic lines, suggesting a retained drain tube (Fig. 1). The lateral soft tissue neck radiograph demonstrated a radio-opaque drain tube in the anterior neck (Fig. 2).
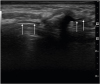 | Fig. 1The longitudinal neck ultrasonography shows a hypoechoic lesion with internal echogenic parallel lines (arrows), suggesting a retained drainage tube.
|
 | Fig. 2The lateral soft tissue neck radiograph displays a Penrose drain fragment (arrows) in the anterior neck.
|
A retained drainage tube formed a mass. So, removal of the drainage tube fragment was performed under local anesthesia. After the surgery, the operation site healed without any complications.
DISCUSSION
Although a clear benefit is lacking, draining the neck after thyroid surgery is still frequently performed for the quick detection of bleeding or the drainage of lymphatic fluid (1). Disadvantages associated with drainage tubes are numerous such as an increased incidence of wound infections (2), more hospitalization days (12), and cosmetic problems. At some hospitals, they sometimes put the Penrose drainage tube in the wound for cosmetic effects. One of the complications associated with the use of Penrose drains occurs when the drain tube breaks, leaving a fragment at the time of the removal attempt. Some cases described retained or tethered Penrose drains after cholecystectomy (3), breast abscess treatment (4), ovarian cancer surgery (5), lower limb amputation (6), and ureteral diversion (7). We have been unable to locate a similar case in the literature whereby a retained Penrose drain was detected as a mass after thyroidectomy.
When a palpable neck mass is detected during the follow-up after thyroid cancer surgery, local tumor recurrence is suspected first. In rare cases, a suture granuloma (8) and benign lymph nodes must be considered. An additional imaging study is needed to evaluate the mass and positron emission tomography scans might be sometimes performed to detect recurrent thyroid cancer. Fortunately, we can diagnose a retained drainage tube with just neck US and a lateral soft tissue neck radiograph. The remnant drainage tube adhered to nearby tissues and was detected as a palpable mass on the neck. Its removal was relatively simple under the local anesthesia.
Recent studies show that a routine drainage following thyroid surgery does not reduce post-operative complications (1). However, a drainage is necessary in complicated cases or when the dead space is very large.
We report the first case of a retained drainage tube fragment in the anterior neck following conventional thyroid surgery with interesting imaging findings. In conclusion, a drainage procedure during thyroidectomy is regarded to be simple and safe. However, surgeons should be aware of associated rare complications and devote more attention to inserting and removing a drainage tube located in the thyroidectomy cavity.
 XML Download
XML Download