

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Poorly differentiated thyroid carcinoma (PDTC) was first described by Sakamoto et al. (1) in 1983. Currently, PDTC is defined by a combination of architectural and cytomorphologic features resulting from the 2004 World Health Organization (WHO) classification and more precisely specified by the 2006 Turin consensus meeting. The histologic and cytologic aspects are detailed with a focus on key features helpful in the diagnosis of PDTC, both using surgical pathologic examinations and in cytology-based studies (2). PDTC exhibits intermediate behaviors between well-differentiated thyroid carcinoma and anaplastic thyroid carcinoma (13456).
Here, we report the case of an extremely rare metastasis to the esophageal submucosa after the first treatment cycle for PDTC.
CASE REPORT
A 68-year-old woman was referred to us in March of 2014 following a thyroidectomy for 2 thyroid nodules (Fig. 1). At the time this patient was referred to us, her fine needle aspiration cytology (FNAC) result showed favor nodular hyperplasia in the left huge thyroid nodule and papillary carcinoma in the right small thyroid nodule. However, when the cytology sample which was obtained by FNAC, was re-examined, it was concluded that it appeared more like a papillary carcinoma rather than favor nodular hyperplasia in the left thyroid and papillary carcinoma in the right thyroid (Fig. 2). The sample had very little cellularity, making the diagnosis very difficult. However, it showed mitosis and nuclear inclusion. Therefore, the clinic pathologist concluded that it was papillary carcinoma. The patient has no past medical history and familial history.
Fig. 1
Pre-operative thyroid ultrasound and CT scan. Right thyroid nodule shows a small central calcification in the upper aspect (blue arrow). Left lobe showed a large 5.2-cm mixed complex type mass of the whole thyroid (white arrow).
CT = computed tomography.

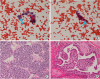
Fig. 2
(A) FNAC slide in left thyroid huge mass: intranuclear inclusions. And very few cellularity (×400). (B) FNAC slid in right thyroid mass: intranuclear inclusion (×400). (C) Insular type PDTC in left thyroid (×200). (D) Papillary thyroid carcinoma in right thyroid (×200).
FNAC = fine needle aspiration cytology; PDTC = poorly differentiated thyroid carcinoma.
The patient underwent a total thyroidectomy with central nodal dissection after few days later. During surgery, no evidence of extrathyroidal extension was found. A 0.8-cm mass was indicated as a papillary carcinoma without extra-thyroidal extension and a 6×5.2-cm mass was indicated as PDTC with capsule and lymphovascular invasion in the final histopathological reports. The level VI node was positive (3/7) with predominantly follicular features. Postoperatively, the patient received radioactive iodine (RAI) ablation (100 mCi) in July 2014. An iodine-131 whole-body scan was performed and indicated no residual lesion was present. Additionally, a postoperative positron emission tomography (PET)-computed tomography (CT) evaluation showed no residual lesion and no recurrence.
The patient was asymptomatic and undergoing regular follow-up until December 2015 when upper gastrointestinal endoscopy during a regular medical follow-up revealed a 2.5×2.0-cm irregular head and pedunculated polypoid mass with friability and luminal narrowing in the mid-upper esophagus, 22-cm from her incisors. This patient continued endoscopic follow-up annually for her health, and had no symptoms such as swallowing difficulty or dysphagia due to the esophageal mass. The biopsy was consistent with metastatic PDTC (Fig. 3). Evaluation was planned for patient condition using chest CT scanning, head and neck ultrasound, laboratory testing, and PET-CT scanning. A chest CT revealed a solitary submucosal lesion in the upper thoracic esophagus and multiple nodular densities that appeared as metastasis in both lung fields (Fig. 4). The head and neck ultrasonography revealed a 2-cm ill-defined marginated irregular shaped hypoechoic mass in the left thyroidectomy bed site and a 1.7×2.3-cm circumscribed oval-shaped enlarged hypoechoic nodule in the left level IV area (Fig. 4). It appeared as a possible thyroid carcinoma recurrence, with a biopsy of consistent with metastatic PDTC. A PET-CT scan also showed uptake localized to the thyroid operation site and upper mid-portion of the esophagus, and multiple pulmonary nodules in both lungs (Fig. 5). The patient's serum thyroglobulin (TG) became surge (1,362.7 ng/mL). At the last follow-up, TG was normal range before this event (15.94 ng/mL). Other thyroid function test results were normal.
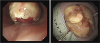
Fig. 4
(A) Esophageal protruding mass (blue arrow). (B) Both lung metastases (blue arrows). (C, D) Post-thyroidectomy site recurrent lymph node enlargement at 18 months (white arrows).

Fig. 5
PET-CT scan. Uptake of post-thyroidectomy site recurrent lymph node (white arrow) and esophageal metastasis (blue arrows).
PET = positron emission tomography; CT = computed tomography.

A modified radical neck dissection was planned after endoscopic esophageal mass resection as palliative treatment to improve the patient's quality of life. This decision was made as metastases were found in both lung fields, and the patient's general nutritional condition was not good. The patient underwent an endoscopic mucosal resection of the esophageal mass in February 2016. The pathology and immunohistochemistry (IHC) profile were suggestive of a 3.0×2.0×1.2-cm lesion of the upper thoracic esophagus with features of metastatic PDTC with involvement of the previously resected margins. IHC staining showed that the tumor was positive for cytokeratin 903 (CK903), galectin-3, AE1/3, vimentin, thyroid transcription factor-1 (TTF-1), TG, and negative for periodic acid-Schiff (PAS), periodic acid-Schiff diastase (D-PAS), and Alcian blue. The patient underwent a modified radical neck dissection for the recurrent thyroid nodules after endoscopic esophageal mass resection 1 week later. The final histopathological diagnosis of the surgical specimen revealed multiple lymph nodes, which were identified as metastatic PDTC. IHC staining revealed that the tumor was positive for 3-fucosyl-N-acetyl-lactosamine (CD15), TG, CK19, E-cadherin, and TTF-1, and negative for CK903. Postoperatively, the patient was administered liothyronine sodium levothyroxine suppression therapy and received RAI ablation (200 mCi) in March 2016. However, we could not evaluate the patient's delayed uptake images, because she could not visit the clinic owing to her femur fracture. The patient is now asymptomatic and has regular follow-ups.
DISCUSSION
PDTC is very rare; it constitutes 2%–10% of all thyroid carcinoma (789) and tumors are of intermediate biological aggressiveness between well-differentiated thyroid carcinoma and anaplastic thyroid carcinoma (7). FNAC is a very useful technique for the preoperative evaluation of thyroid nodules. However, PDTC on cytology has overlapping features between medullary thyroid carcinoma and differentiated thyroid carcinoma on FNAC; therefore, the cytologic findings do not permit a definitive diagnosis of PDTC. Additionally, one study reported that –24% of patients with PDTC showed papillary carcinoma on cytologic analysis before surgery. Most reported a follicular variant of papillary carcinoma (10). This patient's FNAC slide had very little cellularity, rendering the decision challenging for the clinical team.
This thyroid carcinoma subtype has a propensity to metastasize to regional lymph nodes (50%–85%), as well as distantly (36%–85%), most commonly to the lungs and bones (11). Another study reported that distant metastases and local recurrences to be quite variable in patients with PDTC (12). The esophagus is rarely implicated as a site of distant metastasis in thyroid carcinoma. Direct extension is the most common route when metastasis occurs from the primary cancer lesion to the esophagus (13). However, esophageal metastasis was rarely reported during follow-up for an unusual protruding submucosal esophageal tumor. All thyroid cancer subtypes have been reported to be involved in esophageal metastasis. The recurrence intervals were variable from 3 years after the first treatment to 10 years after the first treatment. The most common symptom was dysphasia and, in some cases, hematemesis (13141516).
In this case, local recurrence and submucosal esophageal distant metastasis were examined after 18 months from the first surgical treatment and RAI treatment. To the best of our knowledge, there has only been 1 other case of PDTC metastasis involving the esophagus. Especially, the first follow-up study that was performed 6 months after the first treatment showed no evidence of the disease. However, 1 year later, we assessed serum TG and found it to be elevated; thereafter, we found a metastatic site by ultrasound and esophagogastroduodenoscopy.
Therefore, physicians carefully screened a patient with PDTC during follow-up after the first treatment and found recurrence of the disease. Physicians must consider thyroid cancer history or thyroid evaluation if the patient complains of dysphasia or an esophageal mass is incidentally found.
 XML Download
XML Download