

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Papillary thyroid carcinomas (PTCs) are the most common type of thyroid cancers and account for approximately 75%–85% of thyroid malignancies (1). According to the World Health Organization (WHO) classification system, papillary thyroid microcarcinomas (PTMCs) are PTCs that are 1 cm or less in diameter (2). The prevalence rate of PTCs and PTMCs has recently increased. However, it does not reflect the actual increase of incidence rate itself. This phenomenon could be explained by the early detection of small-sized thyroid tumors through advanced diagnostic tools, such as thyroid ultrasonography and fine-needle aspiration (FNA) cytology (34).
Despite relatively good prognosis, with slow progression and high survival rate, several studies have reported recurrences and metastases in PTMCs (5), the most common of which is metastasis to the central lymph node of cervical neck (67). Given that central neck lymph node metastasis (CLNM) is the most significant risk factor in predicting locoregional recurrences (489), therapeutic central neck dissection is necessary if CLNM is detected in preoperative examination (10). However, whether prophylactic central neck lymph node dissection (CLND) improves survival rate and prognosis in patients without confirmed CLNM in preoperative examination is yet to be determined.
Given that accurate detection of CLNM via thyroid ultrasonography is challenging due to its anatomical structure (11), establishing factors that can be used in predicting CLNM is necessary. This study aims to determine the predictive factors of CLNM that can be used in preoperative patient evaluation and in determining the necessary extent of surgery.
METHODS
In this retrospective single-center study, 625 PTMC patients who underwent thyroid surgery at Chosun University Hospital from January 2002 to December 2012 were evaluated. Three types of surgery, namely, lobectomy, near-total thyroidectomy, and total thyroidectomy were performed.
Preoperative ultrasonography and FNA cytology results of the patients were reviewed, and of these, 575 patients were included in this study according to the following criteria: 1) tumor size of 1 cm or less in diameter, 2) no evidence of CLNM, and 3) diagnosis of PTC through FNA. All patients underwent ipsilateral or bilateral prophylactic CLND along with thyroid surgery according to the tumor location. Total or near-total thyroidectomy with bilateral CLND was performed in case of bilateral tumors and suspicious extra-thyroidal extension in preoperative ultrasonography, and lobectomy with unilateral CLND was performed in case of unilateral and intra-thyroidal tumor.
The medical records and postoperative pathologic reports of all the patients were reviewed, and the results were analyzed with respect to sex; location, number, and size of tumors; type of operation; capsular invasion; lymphovascular invasion (LVI); and recurrence. According to the postoperative pathologic results, the patients were divided into 2 groups; one with CLNM and the other without CLNM. Then, univariate and multivariate analyses of the correlation between CLNM and other clinicopathological features were conducted.
SPSS ver. 21.0 (SPSS Inc., Chicago, IL, USA) was used for statistical analyses. Pearson's χ2 test or Fisher's exact test was used for univariate analysis, and logistic regression analysis was used for multivariate analysis. Along with 95% confidence interval (CI), a P value of <0.05 was considered statistically significant.
RESULTS
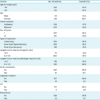
Mean follow-up periods were 109.4 months (range 43–168 months). A total of 262 patients (45.6%) out of the 575 were under 45 years of age, and 516 (89.7%) were female. Unilateral tumors were observed in 329 patients (57.2%), and multifocality (2 or more tumors) was observed in 291 patients (50.6%). In terms of tumor size, 383 cases (66.6%) of tumors larger than 0.5 cm and smaller than 1 cm in size were noted according to final biopsy results. Capsular invasion occurred in 18 patients (3.1%), and LVI was observed in 4 patients (3.1%). Recurrence was observed in 12 patients (2.1%), and all of the recurrences were lateral neck lymph node metastasis (Table 1).
Table 1
Clinicopathologic features in patients with PTMC without suspicious lymph node metastasis on preoperative ultrasonography (n=575)
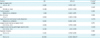
Out of 575 patients, 81 (14.1%) who had no evidence of CLNM in preoperative ultrasonography were confirmed to have CLNM in the postoperative pathologic examination. Median number of metastasis was 2 (range 1–5). By analyzing the correlation between CLNM and each factors mentioned previously, tumor size larger than 0.5 cm and LVI showed statistically significant correlation, with a P value of <0.05. Recurrence during follow-up periods was more frequently observed in patients with CLNM with statistically significant difference (Table 2).
Table 2
Comparison of the factors according to lymph node metastasis in patients with PTMC without suspicious lymph node metastasis on preoperative ultrasonography (n=575)

In multivariate analysis using logistic regression, CLNM risk was higher in men than in women (odds ratio [OR], 0.498; 95% CI, 0.250–0.992; P=0.047). Tumor size (≤0.5 cm) (OR, 2.450; 95% CI, 1.313–4.570; P=0.005) and LVI (OR, 24.954; 95% CI, 2.430–256.217; P=0.007) were statistically significant associated factors (Table 3).
Table 3
Multivariate analysis of factors for central lymph node metastasis in patients with PTMC without suspicious lymph node metastasis on preoperative ultrasonography
DISCUSSION
PTMC has good disease prognosis, with a 10-year disease-specific survival rate of up to 99.5%. Therefore, the aim should be not only to improve survival rate through simple treatments but also to improve quality of life of the patient after treatment.
Given that CLNM is among the most significant risk factors in predicting locoregional recurrences (489), the American Thyroid Association (ATA) strongly recommends therapeutic central neck dissection in PTMCs with evidence of CLNM (10). However, diagnosing CLNM only through preoperative imaging is difficult.
According to Hwang and Orloff (11) and Choi et al. (12), the sensitivity in predicting CLNM through preoperative ultrasonography is low (approximately 23.0%–53.2%). This value indicates a high possibility of false-negative results in imaging, resulting in insufficient treatment of patients who require central neck dissections. In this study, 14.1% of CLNM-negative patients in preoperative ultrasonography were diagnosed to have CLNM according to the final biopsy result.
Therefore, performing prophylactic central neck dissection is debated (131415). Former studies reported transient or permanent hypoparathyroidism and recurrent laryngeal nerve injury as complications of central neck dissection. These complications could degrade the patient quality of life of after surgery (16). If the risk factors of CLNM in PTMCs can be determined, then surgeons can selectively require prophylactic central neck dissection in high-risk patients. As such, unnecessary treatments that might lead to possible complications can be avoided.
Given that age, sex, tumor size, tumor multifocality, and capsular invasion affect PTMC prognosis, these factors were analyzed in our study.
The correlation between age and CLNM is still controversial. Qu et al. (17) reported that the risk of CLNM increases in patients under 45 years of age; however, Lim et al. (18) and Roh et al. (19) reported no statistical significance between age and CLNM. Meanwhile, several researchers claim that performing prophylactic central neck dissection in patients older than 45 years of age results in good prognosis, citing the American Joint Committee on Cancer (AJCC) cancer staging manual that states that PTMC in patients with CLNM older than 45 years of age progresses to stage III and that mortality risk increases in this age group (20). The decreased effectiveness of additional radioactive iodine (RAI) treatment due to decreased RAI uptake ability is also speculated to result in poor prognosis in aging patients. However, the recently revised ATA guideline states that RAI treatment does not provide a significant therapeutic gain in PTMCs (1021). Therefore, this treatment is not definitive. In our study, no statistical significance was noted between age and CLNM.
In general, PTMC is more prevalent in women than in men; however, studies reported that CLNM occurs more frequently in men (2223). In this study, univariate analysis showed no statistical significance between sex and CLNM. However, multivariate analysis showed higher CLNM risk in male population (OR, 0.498; 95% CI, 0.250–0.992; P=0.047). This result suggests that more thorough preoperative examinations and an aggressive recommendation of prophylactic central neck dissection are necessary in male PTMC patients.
Bilaterality and multifocality are risk factors that have consistently been studied. Several studies reported that the tumor recurrence rate increases in multifocal tumors (2425). In one study, the risk of CLNM is higher in bilateral tumor because of the tendency of large tumor size and more frequent extrathyroidal invasions (2627). However, according to Zhao et al. (28), not only multifocality but both tumor size and multifocality are considered to be related to CLNM. In this study, neither location nor number of tumor showed statistically significant correlation to CLNM.
Meanwhile, tumor size was observed to be an important factor in predicting CLNM, and this result corresponds to that of several recent studies (2930). Although a large tumor is associated with poor prognosis in PTC patients, some studies reported no significant difference in prognosis related to tumor size (≥0.5 vs. <0.5 cm) (3132). However, we still consider tumor size to be a significant independent predictive factor of CLNM because our study is concerned with the overall mortality and tumor recurrences.
The correlation between capsular invasion and CLNM and between LVI and CLNM is also controversial. Although univariate and multivariate analyses indicated no correlation between capsular invasion and CLNM in this study, Kim et al. (33) reported otherwise. However, the proportion of patients with confirmed invasion was over 50% in Kim et al.'s study (33) and was only 3.1% in our study. This difference may have resulted from varying methods of histopathologic examination and the criteria of defining the invasion in each center.
LVI and CLNM showed a significant correlation in our study, similar to the result of Joo et al. (3435) but different from that of Roh et al. (19). Considering the anatomical structure of thyroid gland and its well-developed lymphovascular structure that drains primarily to cervical lymph node (36), our result of a correlation between LVI and CLNM is logical. Arora et al. (35) reported that the incidence of LVI in PTMC was 6.1% (4 patients in total 66 patients). LVI was very low in our study, and further investigation is necessary with more patients.
CONCLUSION
Male sex, large tumor size, and LVI were found to be risk factors that can be used in detecting CLNM in PTMC patients who had no preoperative clinical evidence of CLNM. However, there is a limitation that we cannot confirm the LVI before surgery. So, further investigation should be performed to predict a CLNM in PTMC with available factors before surgery.
 XML Download
XML Download