

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Hypocalcemia is the most common and sometimes the most severe postoperative complication of total thyroidectomy (1). It is defined as ionized calcium (iCa) levels that remain under 1.0 mmol/L or the development of clinical symptoms and signs (2). Hypocalcemia often increases the duration of hospital stay, overall cost of a thyroidectomy, need for frequent biochemical tests, and frequency of emergency room visit (3). It causes symptoms ranging from mild paresthesia and tingling to more severe tetany and convulsions (4). The incidence of transient hypoparathyroidism is 10%–30% and the rates of permanent hypoparathyroidism as high as 1%–2% has been reported (5).
The early identification of patients at risk of hypoparathyroidism after total thyroidectomy helps to determine who would benefit from early calcium (Ca) supplementation (6), thereby, reducing the discomfort associated with many blood tests and high treatment costs (7). Thus, it is important to identify individuals at risk of hypoparathyroidism after total thyroidectomy with high accuracy. However, the optimal approach for this remains poorly defined (8). Various protocols for diagnosing and managing post-thyroidectomy hypocalcemia have been reported (9). The conventional approach, which consists of clinical assessment and monitoring of serum Ca levels, is still commonly used (10). However, more recently, measurements of serum intact parathyroid hormone (iPTH) have been used to predict which patients are at risk of hypoparathyroidism after thyroidectomy (11). To ensure accurate prediction, it is important to determine the optimal time for measuring iPTH. Various studies have assessed the usefulness of iPTH measurements obtained during surgery, at 1, 4, and 6 hour intervals after surgery, and on the morning of postoperative day 1 (121314). Nevertheless, the time point of iPTH measurement that best predicts the parathyroid function prognosis of patients remains unclear (15).
This retrospective cohort study was performed to identify the optimal time point for measuring iPTH, namely, the time point that most accurately and efficiently predicts the development of hypoparathyroidism after total thyroidectomy. We also determined the postoperative day 1 iPTH level that best and most safely predicted the development of permanent hypoparathyroidism after total thyroidectomy.
METHODS
1. Patients
All consecutive patients who underwent total thyroidectomy in a single center between January 2013 and January 2015 and were followed up for at least 12 months were reviewed. The following data were extracted: patient age and sex, tumor size, indication for surgery (benign vs. malignant lesion), extent of surgery (simultaneous central and/or lateral neck dissection), and the iPTH and Ca levels measured at 2 hours after surgery, and on postoperative days 1 and 2, and 12 months after surgery.
2. Surgical procedure
All surgical procedures were performed by a single experienced endocrine surgeon. Patients who underwent both conventional open thyroidectomy and Bilateral Axillo-Breast Approach (BABA) robotic thyroidectomy were included in the study. BABA robotic thyroid surgery consists of endoscopic surgery with a robot system (16). In cases of proven malignant thyroid carcinoma underwent prophylactic ipsilateral central neck lymph node dissection. Modified radical neck dissection was performed when lateral neck lymph nodes metastasis was proven on pathological confirmation. In all cases, efforts were made to identify and preserve all of the parathyroid glands. Thus, the parathyroid gland dissection, separation of the glands from the thyroid capsule, and preservation of the parathyroid arteries were all performed carefully. Since the position of the superior parathyroid glands is constant but that of the inferior parathyroids is much more variable (17), the surgical approach was based on a thorough knowledge of the embryological development of the parathyroid glands.
3. Treatment protocols and management of hypocalcemia
Patients were usually admitted a day before or on the day of operation and were routinely discharged on the second postoperative day if they did not exhibit severe complications after the thyroidectomy. If patients had clinical symptoms of hypocalcemia and iPTH level of <15 pg/mL after total thyroidectomy, they were started on medication, as follows. If symptomatic hypocalcemia developed during hospitalization, an intravenous infusion of calcium gluconate (1 mg/kg/hr) was administered. Patients with iPTH levels between 10 and 15 pg/mL began oral calcium carbonate (500 mg of elemental Ca 2T bid) and hydroxycholecalciferol (0.5 μg 2T qd) treatment. Patients with iPTH levels <10 pg/mL were usually treated with oral Ca (500 mg of elemental Ca 2T qid) and hydroxycholecalciferol (0.5 μg 2T qd–bid). The oral Ca and hydroxycholecalciferol were later tapered on an outpatient basis.
4. Definitions of transient and permanent hypoparathyroidism and laboratory findings
The total serum Ca levels (including iCa levels), and iPTH levels were measured at 2 hours after surgery and on postoperative days 1 and 2. We considered that iPTH level on postoperative day 2 is a true iPTH status of the patient and can determine transient hypoparathyroidism. The patients then visited the clinic 2 weeks after the operation for routine check, and thereafter were regularly followed up at 3–6 month intervals. Serum Ca levels, iCa levels, and iPTH levels were measured 3 and 12 months postoperatively. iPTH was measured using the Roche modular E170 System electrochemiluminescence immunoassay (Roche Diagnostics Ltd., Rotkreuz, Switzerland). The normal iPTH level in our laboratory ranges from 15 to 65 pg/mL. Transient postoperative hypoparathyroidism was defined as an iPTH level on the second postoperative day of <15 pg/mL. Permanent hypoparathyroidism was defined as absolute iPTH values of <15 pg/mL that lasted 12 months or longer, thus requiring long-term Ca supplementation.
5. Statistical analysis
The continuous demographic and clinical variables were expressed as mean (standard deviation) or as median (interquartile range). The categorical demographic and clinical variables were expressed as number (percentage). Correlations between iPTH levels at the various time points were assessed using Pearson's correlation analysis. Receiver operating characteristic (ROC) curve analysis was used to identify the postoperative day 1 iPTH cutoff levels for permanent hypoparathyroidism. Statistical analysis was performed using SPSS version 22.0 (Statistical Package for Social Sciences; SPSS Inc., Chicago, IL, USA). P values of <0.05 were considered to indicate statistical significance. All patients provided written informed consent for the study. This retrospective cohort study was approved by the Institutional Review Board (Approval No. B-1603-338-111).
RESULTS
1. Patient characteristics
In total, 730 patients who underwent total thyroidectomy with or without lymph node dissection and were followed up for at least 12 months during the study period were enrolled. The median age was 47.2 (range, 34–59) years and 549 (75.2%) were female. The mean tumor size was 1.2±0.8 cm. Eighteen patients (18/730, 2.5%) underwent total thyroidectomy alone, 578 (578/730, 79.2%) underwent total thyroidectomy with central lymph node dissection, and 134 (134/730, 18.3%) underwent total thyroidectomy with modified radical neck dissection. The preoperative diagnosis was papillary thyroid carcinoma (n=673, 92.2%), medullary thyroid carcinoma (n=15, 2.1%), follicular thyroid carcinoma (n=7, 0.9%), and others (n=35, 4.8%), including Graves' disease, benign huge goiter, and bilateral follicular adenoma.
Of the 730 patients, 237 (237/730, 32.5%) had transient hypoparathyroidism, as defined by a serum iPTH level of <15 pg/mL on the second postoperative day. Twenty-eight patients (28/730, 3.8%) developed permanent hypoparathyroidism, as indicated by the iPTH levels 12 months after surgery. These patients required long-term oral Ca supplementation (Table 1).
Table 1
Clinical characteristics of the patients

CND = central neck dissection; MRND = modified radical neck dissection; iPTH = intact parathyroid hormone.
*Transient hypoparathyroidism was defined as a serum iPTH level of <15 pg/mL on postoperative day 2. †Permanent hypoparathyroidism was defined as a serum iPTH level of <15 pg/mL 12 months after surgery.
2. Correlations between postoperative iPTH levels at 2 hours after surgery, on postoperative days 1 and 2, and 12 months after surgery
While the iPTH level on postoperative day 2 correlated strongly with the iPTH level 2 hours after surgery (Pearson's correlation, r=0.786; P<0.001), it correlated more strongly with the iPTH level on the first postoperative day (r=0.915; P<0.001) (Fig. 1A and B). Thus, when transient hypoparathyroidism is defined as iPTH levels <15 pg/mL on postoperative day 2, the iPTH level on postoperative day 1 is a better predictor of transient hypoparathyroidism than the iPTH values at 2 hours after surgery.
Fig. 1
Correlations between the iPTH levels (A) at 2 hours after surgery and on postoperative days 2 (r=0.786; P<0.001), (B) on days 1 and 2 (r=0.915, P<0.001), (C) at 2 hours after surgery and 12 months (r=0.258; P<0.001), and (D) on day 1 and at 12 months (r=0.277, P<0.001).
iPTH = intact parathyroid hormone.

Of the 730 patients, 52 (52/730, 7.1%) had discrepant iPTH levels 2 hours after surgery and on postoperative day 1. Of these 52 patients, 14 (14/52, 26.9%) had a normal iPTH level at 2 hours after surgery, but this level was <15 pg/mL on postoperative days 1 and 2. Of these 14 patients, 1 (1/14, 7.1%) developed permanent hypoparathyroidism. Thus, if the clinician had relied on only the measurement at 2 hours after operation to predict hypoparathyroidism, 14 patients with potential hypocalcemic symptoms would have been discharged without Ca supplementation, which could have been dangerous. The remaining 38 patients (38/52, 73.1%) who had discrepant iPTH levels 2 hours after surgery and on postoperative day 1 exhibited iPTH levels of <15 pg/mL 2 hours after surgery but normal levels on postoperative days 1 and 2. None of these 38 patients developed permanent hypoparathyroidism (Table 2). Mean serum iCa level of the patients with and without transient hypoparathyroidism on postoperative day 1 was 1.07±0.075 mmol/L and 0.97±0.091 mmol/L, respectively (P=0.492)
Table 2
Clinical course of the patients with discrepant serum iPTH levels 2 hours after surgery and on postoperative day 1

The iPTH levels 12 months after surgery correlated significantly and positively with the iPTH levels 2 hours after surgery and on postoperative day 1 (r=0.258; P<0.001 and r=0.277; P<0.001, respectively) (Fig. 1C and D).
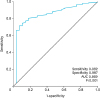
3. Identification of the postoperative day 1 iPTH level that best predicts permanent hypoparathyroidism
ROC curve analysis was used to identify the iPTH level that best predicted permanent hypoparathyroidism. The postoperative day 1 iPTH level of 3.05 pg/mL predicted permanent hypoparathyroidism with a sensitivity of 92.9% and a specificity of 99.7%. The patients were then divided according to whether their postoperative day 1 iPTH level was < or ≥3.05 pg/mL (Fig. 2). All but 13 of the patients with postoperative day 1 iPTH levels of <3.05 pg/mL developed permanent hypoparathyroidism. Adequate Ca supplementation is indicated in this group. The safest cutoff value of postoperative day 1 iPTH levels for permanent hypoparathyroidism was 9.65 pg/mL, which predicted permanent hypoparathyroidism with a sensitivity of 70.9% and a specificity of 100%. None of the patients with a postoperative day 1 iPTH level of >9.65 pg/mL had permanent hypoparathyroidism 12 months after surgery.
DISCUSSION
Parathyroid dysfunction that leads to symptomatic hypocalcemia after total thyroidectomy is a major concern. The clinical manifestations of hypoparathyroidism after thyroidectomy depend on the extent of hypocalcemia and the rapidity of hypocalcemia onset (18). Patients with transient hypocalcemia may present with symptoms that range from mild (such as numbness of the distal extremities, circumoral paresthesia, and carpopedal spasm) to severe (such as confusion, delirium, and seizure) (18). Manifestations of chronic hypocalcemia include basal ganglia calcifications, cataracts, and dental abnormalities (192021).
Although hypoparathyroidism after total thyroidectomy reverses spontaneously within a few months in most cases, in a few patients, it persists for more than 1 year and must be considered permanent. In these cases, to avoid the subtle but potentially lethal complications of chronic hypocalcemia, lifelong therapy and follow-up are mandatory. However, long-term Ca supplementation can also cause substantial discomfort and various side effects, including gastrointestinal side effects (mainly constipation), renal calculi, and myocardial infarction (22).
The parathyroid insufficiency that leads to postsurgical hypocalcemia is due to intraoperative damage to the parathyroid glands that is caused by mechanical or thermal trauma, accidental resection, and/or, most commonly, parathyroid devascularization (23). To minimize parathyroid injury, many surgical techniques have been developed and a variety of techniques have been used such as intraoperative carbon nanoparticles injections, methylene blue infusion, technetium-99m-sestamibi localization using a hand-held gamma probe, and optical coherence tomography (24252627).
Several recent studies evaluated the ability of early postoperative iPTH levels to predict hypocalcemia. Grodski and Farrell (28) prospectively investigated 76 patients undergoing total or completion thyroidectomy by monitoring the iPTH levels between 4 and 12 hours after surgery. They concluded that a single parathyroid hormone (PTH) measurement at this time point accurately predicts the patients who are at risk of hypocalcemia. Lombardi et al. (12) also evaluated the early postoperative iPTH levels as an indicator of post-thyroidectomy hypocalcemia. They found that an iPTH level of <10 pg/mL 4 or 6 hours after surgery predicted postoperative hypocalcemia with a specificity of 100%, a sensitivity of 94%, and an overall accuracy of 98%.
However, the results of the present study showed that the iPTH levels 2 hours after surgery were not appropriate as an indicator of postoperative hypoparathyroidism: there were 52 patients (52/730, 7.1%) whose iPTH levels 2 hours after surgery and on postoperative day 1 did not coincide. Of these 52 patients, 14 (14/52, 26.9%) had normal iPTH levels at 2 hours after surgery but had iPTH <15 pg/mL on the first postoperative day. If the iPTH levels taken 2 hours after surgery had been used to determine postoperative hypoparathyroidism, these patients would not have been given Ca supplementation and thus could have been at risk of hypocalcemia after surgery. Although postoperative hypocalcemia is self-limiting in most patients, if it is not properly treated, it can result in the most severe complications that are associated with total thyroidectomy. The remaining 38 patients (38/52, 73.1%) who had discrepant iPTH levels 2 hours after surgery and on days 1 exhibited low iPTH values at 2 hours after surgery that recovered to normal by the first postoperative day. Thus, in these patients, it may be unnecessary to administer Ca and hydroxycholecalciferol supplementation. Several studies describe that iPTH level at 6 hours after surgery is a good predictor of hypoparathyroidism. Even though iPTH levels at 6 hours after surgery has a value of predictor, it is difficult to obtain 6–12 hour postoperative iPTH levels, because the results are usually obtained in the evening or at night on the day of surgery.
By contrast, the present study showed that a single iPTH measurement on postoperative day 1 can accurately predict which patients are at risk of transient and permanent hypoparathyroidism after total thyroidectomy. This is because transient hypoparathyroidism is defined as a serum iPTH level of <15 pg/mL on the second postoperative day and the postoperative day 1 iPTH levels correlated particularly strongly with the postoperative day 2 levels. Moreover, postoperative day 1 iPTH value predicted permanent hypoparathyroidism with a high sensitivity and specificity.
Several studies support the use of postoperative day 1 iPTH levels for identifying patients at risk of hypoparathyroidism after thyroidectomy. Cayo et al. (14) measured iPTH levels on the morning of postoperative day 1 and found that iPTH levels below 10 pg/mL accurately identified patients at risk of clinically significant hypocalcemia (odds ratio, 1.08). Moreover, in a retrospective study, Wang et al. (29) found that postoperative day 1 iPTH levels of <5.0 pg/mL predicted the need for vitamin D supplementation for more than 1 month with a positive predictive value of 27%, sensitivity of 100%, and specificity of 80%. They suggested that serum iPTH levels obtained on the morning of the first postoperative day after total thyroidectomy may predict the development of hypocalcemia that requires vitamin D supplementation.
The limitation of using postoperative day 1 iPTH levels to predict clinically significant postoperative hypocalcemia is that it would be difficult to apply this protocol when seeking to discharge patients on the operative day because these values would not be available. Thus, the factors used to predict hypoparathyroidism depend on the medical center. Nevertheless, if postoperative day 1 iPTH values are available, they can serve as an accurate predictor of patients who are at risk of transient or permanent hypoparathyroidism after total thyroidectomy. In an outpatient basis center, however, it will be necessary to routinely prescribe oral Ca to ensure safety and reduce the cost of outpatient thyroid surgery.
We observed that several patients who had normal iPTH levels 2 hours after surgery exhibited a drop in the iPTH levels on the first postoperative day. This can probably be explained as follows. First, when parathyroid function is impaired, the Ca levels reach their nadir 3 days after surgical intervention while iPTH levels are lowest 3 hours after total thyroidectomy (30). Therefore, the normal postoperative iPTH levels at 2 hours after surgery may have reflected the remnant iPTH in the serum before it reached its nadir. Second, intraoperative injury to the parathyroid glands sometimes gradually impairs their function. By contrast, other patients had low iPTH values 2 hours after thyroidectomy but these values then normalized on the first postoperative day. This may reflect the fact that these patients only had relative parathyroid insufficiency that was probably due to temporary vasospasm during operation; in such patients, it is possible for parathyroid function to recover promptly after total thyroidectomy.
We also acknowledge that in many countries, including the United States, patients of thyroid surgery are discharged on the same day of the operation. The strong point of this study, however, lays in the fact that it is not possible to perform a study of this kind in those institutions performing same-day discharge. Based on the results of our study, transient hypoparathyroidism may occur in 26.9% of patients on the following day, even if the normal iPTH levels at 2 hours after the surgery. These patients can suffer mild to severe hypocalcemic symptoms at home which can be lethal sometimes. Therefore, it may be helpful to prescribe Ca supplement as an emergency medicine for patients discharging on the same day of total thyroidectomy.
 XML Download
XML Download