

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Urinary tract infection (UTI) is a common disease among diverse age groups. Many clinicians are confronted with UTIs even in primary healthcare practices, as well as in tertiary medical centers. Its high prevalence rate and morbidity make frequent use of antimicrobials clinically [1]. Antibiotic resistance has been increasing recently, and its seriousness is a global problem. Empirical antimicrobials for the treatment of UTIs should be selected on the basis of epidemiological data, including the characteristics of causative bacteria and the result of susceptibility test in a regional community. Resistant bacteria are constantly evolving, and as such, continuous monitoring of the resistance pattern of uropathogens is important for the establishment of empirical therapy. Fosfomycin has been a recently re-emerging antibiotic, representing the epoxide class of antibiotics. It has been focused in treating infectious diseases from multidrug-resistant Enterobacteriaceae. In this study, the susceptibility pattern of antimicrobials to Escherichia coli from community-acquired uncomplicated UTIs was assessed focusing on fosfomycin.
MATERIALS AND METHODS
To reflect the national status of antimicrobial susceptibility, a nationwide hospital recruitment was accomplished. For the responsible fulfillment of laboratory processes, institutions were selected preferentially among university hospitals that cooperated with the Korean Association of Urogenital Tract Infection and Inflammation (KAUTII). A total of 10 university hospitals covering a vast majority of the country were recruited. Between August and December of 2015, study materials were collected from these hospitals.
The materials of this study were E. coli identified in the usual outpatient clinical process. Mid-stream urine samples from adult female patients, who were diagnosed with community-acquired uncomplicated UTIs in the outpatient clinic, were collected for culture identification before taking any antimicrobials. If E. coli was confirmed as a pathogen, the strain was enrolled in this study. Any complicated UTI cases, including urolithiasis, male patients, indwelling catheter, uncontrolled diabetes mellitus, kidney transplantation, and urogenital anomaly, were excluded. The Institutional Review Board of St. Vincent's Hospital of The Catholic University of Korea approved the study protocol (VC15OIMI0059).
Consistent study guidelines for urine collection, culture, antibiotic susceptibility test, and delivery of bacterial colony were established all institutions that participated. Mid-stream urine of 10 ml was collected in sterile container and was streaked onto the blood and MacConkey agar. After culture at 37℃, all E. coli were characterized on the Vitek® 2 using GN and AST-GN30 cards (BioMérieux, Durham, NC, USA) for routine identification and susceptibility testing.
Presently, fosfomycin susceptibility test was not applicable to the automated system of each designated hospital. For an additional test, the E. coli plates were sealed with plastic film and delivered to the central lab in a cold storage system (Departments of Laboratory Medicine, Chung-Ang University College of Medicine, Seoul, Korea) within 24 hours. The disk diffusion method was used for the susceptibility test of fosfomycin [2]. From the delivered E. coli plate, 1 colony was collected and put into the Muller-Hinton broth. Turbid was adjusted with MacFarland unit 0.5, and the liquid was evenly streaked 3 times with a cotton bud onto the Muller-Hinton agar. Before being dried out, fosfomycin disk was put down on the plate and was cultured overnight at 37℃. The zone diameter interpretation was as follows: Resistant: 12 mm or less, Intermediate: 13-15 mm, and Susceptible: 16 mm or more.
RESULTS
A total of 347 E. coli isolates were collected from the urine cultures. All enrolled patients had community-acquired uncomplicated UTIs that were composed of acute cystitis (84.1%, 292) and acute pyelonephritis (15.9%, 55). All patients were female, and the average age was 46.9 (21-72 years old). The most prevalent comorbidity was diabetes (3.5%, 12). The proportion of patients who had undergone antibiotic treatment for UTI in the past 6 months was 35.7% (124).
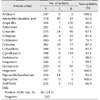
The susceptibility rates of antibiotics were as follows: amikacin 100.0% (347), imipenem 100.0% (347), ciprofloxacin 57.1% (198), cefotaxime 74.9% (260), ampicillin 30.0% (104), trimethoprim/sulfamethoxazole (TMP/SMX) 66.9% (232), and fosfomycin 98.0% (340). The rate of extended-spectrum β-lactamase (ESBL) manifestation was 24.5% (85). Table 1 shows the number of isolates and susceptibility.
Fosfomycin susceptibility was higher than most other antibiotics. Only 7 out of the 347 E. coli isolates were resistant to fosfomycin. All of the fosfomycin-resistant E. coli were ESBL-producing. In 85 cases of ESBL-producing E. coli, the fosfomycin susceptibility rate was 91.8% (78/85). Even in these cases, amikacin and imipenem still showed to be effective. Among patients who provided fosfomycin-resistant strains, 85.7% (6/7) cases had one or more experiences of UTI in the past 6 months.
DISCUSSION
For the establishment of valid guidelines for UTIs, microbiological characteristics, including clinical information about hospital and community acquired infection, should be provided. Particularly for primary health clinic, the guidelines should reflect the data on the community acquired UTI. According to a previous research regarding unresolved acute uncomplicated cystitis, the patient who failed to be treated of UTI at a primary clinic showed high antibiotics resistance rate in the empirical regimen. If the first line antimicrobial, like TMP/SMX or fluoroquinolone seems to be ineffective, a second line antimicrobial should be considered on the basis of local resistance study [3]. Improved surveillance of antibiotic resistance among uropathogens that causes uncomplicated UTIs may help clinicians to make informed decisions about the empirical and alternative treatment of uncomplicated UTIs [4].
Antibiotic resistance has been steadily increasing, and existing empirical treatments of uncomplicated UTI is becoming a problem. The treatment of emerging multidrug resistant (MDR) gram-negative organisms is also becoming a greater challenge. The slow rate of development of newer antimicrobials has led to the re-discovery of the ‘old’ and ‘forgotten’ antibiotics, like colistin and fosfomycin [56]. Fosfomycin was first isolated in 1969 from Streptomyces, which is now produced synthetically [6]. Fosfomycin inhibits the synthesis of peptidoglycan at a step earlier than beta-lactam or glycopeptide antibiotics and has a broad spectrum of activities against various Gram-positive and Gram-negative bacteria, including methicillin-resistant Staphylococcus aureus and vancomycin-resistant enterococci. In the early period of its development, in vitro test of the drug was not able to support in vivo results, and it had been underutilized. Recently, however, fosfomycin received attention as an agent against MDR and has been actively researched [789]. It has been shown to have advantages in treating UTIs due to its high concentration in the urinary tract, exceeding 2,000 mg/L after the initial administration that remains for a prolonged period, over 24 hours [810]. Moreover, fosfomycin has been shown to be very well tolerated and with a low adverse effects, ranging between 1-10% of patients [8].
The clinical evidence of fosfomycin against resistant Gram-negative infections is limited but promising. There have been several clinical studies in Spain, France, and Italy since 1990 [11]. The susceptibility rate of fosfomycin in these countries was revealed to be around 97.4-99.4% [12131415]. Japan has been using fosfomycin for systemic infection, showing high efficacy against several infections; it has remained to be favorable against several bacterial species for more than 20 years [1116].
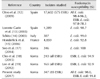
Recently, there have been several studies in South Korea on fosfomycin with respect to UTI treatment. Seo et al. [17] reported in 2014 reported that fosfomycin susceptibility on community-acquired UTI was 100% (346/346). With respect of ESBL control, Cho et al. [18] tested 277 isolates of ESBL-positive E. coli and Klebsiella pneumoniae from urine samples of patients with UTI, and showed that 243 out of the 277 (87.7%) isolates were susceptible to fosfomycin. In another study, a total of 347 non-duplicate ESBL-producing E. coli (165 isolates) and K. pneumoniae (182 isolates) were collected, and the susceptibility to fosfomycin was reported to be 92.9% in E. coli and 95.2% in K. pneumoniae (Table 2) [19].
This study has some limitations. Only tertiary referral hospitals participated in this study. Therefore, theoretically, our results may be inappropriate for full extrapolation to other patient population receiving care in non-tertiary facilities. As a referral hospital, it is possible that some of the enrolled patients with uncomplicated UTIs may have been referred from primary clinics after failed initial antimicrobial treatment. In such patients, the antimicrobial susceptibility was expected to be lower compared with those presenting UTIs without prior exposure to antimicrobial treatment [3].
CONCLUSIONS
Many reports including this study suggest the value of fosfomycin as a useful option for the treatment of community acquired uncomplicated UTIs. To establish the guideline for UTI management, the role of fosfomycin should be reviewed. Further research is necessary to verify the clinical efficacy of fosfomycin as a means to treat UTIs.
 XML Download
XML Download