

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Chronic subdural hematomas (CSDHs), one of the most common types of intracranial hemorrhage, particularly in the elderly, has been reported to have a significant recurrence rate ranging from 9.2 to 26.5%.5,6,9,11,13,18) CSDHs are still a matter for debate, due to controversies in the pathophysiology and surgical treatment.10) Literatures about different surgical techniques and postoperative results of the CSDHs have been published a lot, however, studies regarding the prognosis depending on the patient's postoperative posture are few.1,15) Concerning about the postoperative posture in CSDHs, one group concluded early postoperative upright posture was not associated higher risk of recurrence, but the other group demonstrated quite contradictory conclusion on the early postoperative upright posture. One of the authors of our institute have maintained the lesion side down supine posture tactic postoperatively after burr hole drainage to ease earlier expansion of the compressed brain resulting in less chance of recurrence in CSDHs, and the remaining authors maintained ordinary supine posture. To our best knowledge, we could not find out any study on the effect of head rotation. This retrospective study was carried out to elucidate the efficiency of the lesion side down supine posture over the ordinary supine posture on the recurrence rates and hospital stay.
Materials and Methods
We retrospectively reviewed 78 patients with CSDHs who were treated with burr-hole drainage from August 2005 to April 2011. The CSDH patients included in this study were followed-up for at least 3 months. The exclusion criteria were 1) those with ventriculoperitoneal shunt, 2) subdural hygroma, 3) history of seizure, 4) alcohol abuse, 5) complications after another brain surgery, 6) bilateral subdural hematomas, 7) taking anticoagulant or thrombolytic drugs, 8) two or more burr hole drainage.
All patients underwent one burr-hole surgery with closed system drainage and were then allocated to Group A, who were kept in a lateral position with the operation site downward for 3-5 days after operation, and to Group B, who were kept in supine neutral position. The interval of position change in Group A was defined as 3 hours; three hours with lateral position and one hour with supine position. All the patients were in flat position without head elevation. After 3-5 days, there was no restriction in patients' activities in both groups.
The surgical procedure was as follows. After the burr-hole was made, the dura was opened in a cruciate manner. After catheter insertion, subdural space was liberally irrigated with warm physiological saline solution until the refluxing fluid was clear. Post-operative drains were used. The amount of subdural hematoma drainage was checked every day. When less than 10 cc was drained, we removed the catheter. Postoperative CT scans were checked on postoperative day (POD) 1, POD 3, day of discharge, and on POD 90. The amount of CSDHs was assessed in each group on these postoperative CT scans. Subdural hematoma was categorized into two groups by their thickness in the CT at the POD 3; less and larger than patient's bone thickness.
We defined the recurrence was the re-accumulation of the hematoma in the follow-up brain CT despite of the total resolution of primary subdural hematoma.16,17) Remnant hematoma was defined as the still remained the hematoma in the follow-up brain CT. The reoperation rate and length of hospital stay was assessed in each group.
All statistical analysis was performed by using SPSS 18.0 software (SPSS Inc., Chicago, IL). Independent t-test was used for comparison of continuous variables as patient's age and hospital stay. The cross table analysis was used for nominal data. The level of p<0.05 was considered statistically significant.
Results
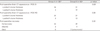
A total of 78 patients met the above criteria and were enrolled in this study (Table 1). Seventy eight patients, 20 females and 58 males, were operated at our institute. Of the 78 patients with CSDHs, 28 (35.9%) were categorized into Group A and 50 (64.1%) into Group B. The patients in this study were 18 to 96 years old.
In Group A, 24 patients (85.7%) were with subdural fluid less than patients' bone thickness. In Group B, 31 patients (62%) were with subdural fluid less than patients' bone thickness. Group A showed earlier brain re-expansion and earlier hematoma drainage (p=0.02).
In Group A, one patient underwent craniotomy due to acute hematoma. This patient recovered without neurologic deficits. In Group B, two patients expired by pneumonia. There was no significant difference between the two groups in patients recovery (p=0.52)(Table 2).
The median days of the hospital stay was 8 days (5-21 days) in Group A and 10 days (5-31 days) in Group B (p=0.01)(Table 1).
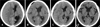
Recurrence was in six patients (7.69%); two (2.56%) in Group A and four (5.13%) in Group B (Figure 1). Recurrence was occurred at one month after operation in three patients and at 2 weeks after operation in three patients. They all underwent reoperation. There were no significant differences between the two groups in recurrence rate (p=0.91)(Table 2).
Discussion
CSDHs are one of the most common surgical problems faced by neurosurgeons. The treatment goal of CSDHs is complete drainage of the collection, using the least invasive technique without a high risk of recurrence. According to previous report, there was no notable difference in the prognosis between single burr-hole and double burr-hole operations.8) Moreover, previous study concluded that there was no notable difference in the prognosis between craniotomy and burr-hole trephination.12)
It is known that the normal intracranial constituents are brain parenchyma, cerebral blood volume and cerebrospinal fluid. These volumes are contained in an inelastic, complete closed skull. We thought that the brain which has been compressed for long time would expand more rapidly if the patient lied in the direction of gravity after hematoma had been removed.
In this study, patients in both group A and B were told not to take sitting position for 3-5 days after operation. Therefore earlier brain re-expansion and consequent shorter hospital stay in Group A suggested the effectiveness of lesion side down posture after CSDH operation.
Several factors have been recognized to increase the risk of CSDHs recurrence after burr-hole surgery.2-4,7,14,16,19) The role of postoperative patient posture in the recurrence of CSDHs has not yet been sufficiently studied. Mehdi A et al.1) also evaluated 84 patients with CSDHs into two groups, each containing 42 patients. The patients in Group A were kept in a supine position for 3 days after the operation, whereas those in Group B assumed a sitting position for the same duration. The recurrence rates in Groups A and B were 2.3 and 19%, respectively. The difference was statistically significant (p=0.02). Therefore, it can be concluded that assuming an upright posture soon after operation is associated with an increased incidence of CSDHs recurrence. However, Nakajima et al.15) reported conflicting findings. They allocated 46 patients with CSDHs into two groups, each containing 23 patients. The recurrence rates in Groups A and B were 14.3 and 16%, respectively. The difference was not statistically significant.

 XML Download
XML Download